In theory, fitting scleral lenses for my dry eye patients was a logical evolution for both my dry eye and rigid gas permeable (RGP) contact lens practice specialities, but there were a few obstacles to making it a success in practice. Time was a significant issue. Dry eye patients typically have numerous return visits, so dragging them back for even more contact lens appointments was a barrier to fitting them with scleral lenses. It also adds to the cost of treatment, which can be quite significant for patients with severe dry eye disease (DED).
Given it can accurately design customised scleral lenses based on an initial topography map, Visionary Optics’ sMap3D seemed a good solution. The corneo-scleral topographer captures three images in different gazes – primary, lower and upper – and combines them into a 3D rendering of the cornea and surrounding sclera (Fig 2) reducing fitting time and thus patient costs.
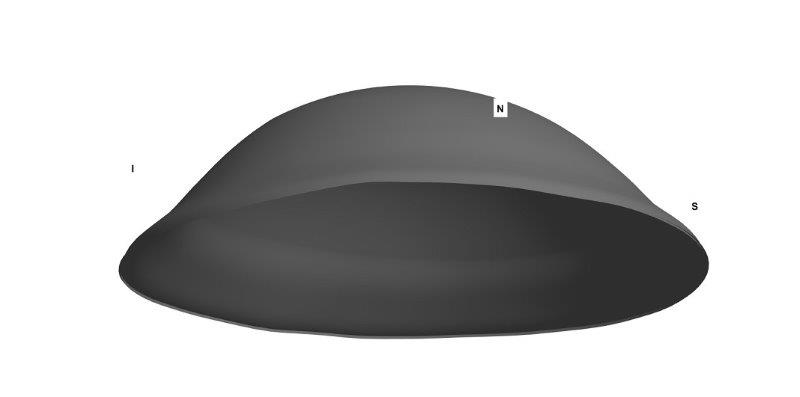
Fig 1. 3D rendering of 16mm scleral lens for right eye
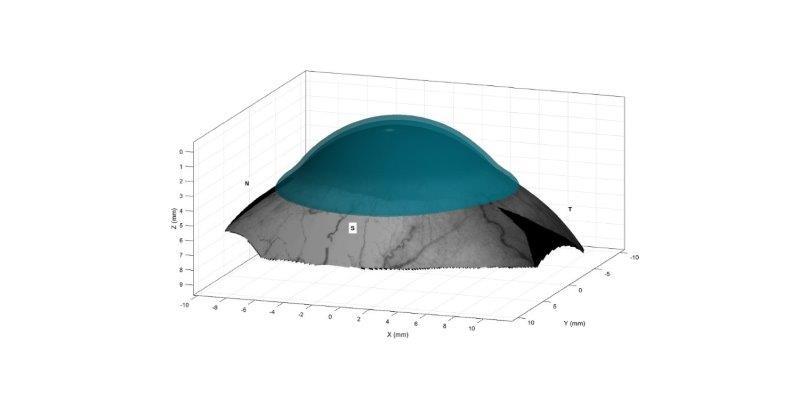
Fig 2. 3D rendering of scleral lens on eye
Scleral lenses
Simply defined, a scleral lens is one that is fitted to vault over the entire cornea, including the limbus, and rests on the conjunctiva overlying the sclera1. Indications for fitting scleral lenses include keratoconus, pellucid marginal degeneration, limbal stem cell deficiency, neurotrophic keratitis and dry eye2.
A 2015 review concluded that scleral lenses are efficacious and well tolerated for use in severe DED6, while the TFOS DEWS II report stated RGP scleral lenses may play an important role in the management of moderate to severe DED, placing scleral lenses as an option within the third step of its staged management algorithm7.
Use of scleral lenses is growing globally3 with eyecare practitioners increasingly considering them as the first-line treatment for patients with keratoconus4. Compared with rigid corneal lenses, scleral lens wearers report greater satisfaction in vision and comfort4 and vision-related quality of life5.
DED case study
One of my patients, a 34-year-old female, is a chronic dry eye sufferer. Although I had successfully treated her symptoms in the past, her administrative job meant long hours of computer work and air conditioning that led to flare-ups. Scleral lenses would keep her eyes hydrated and protect her ocular surface from the dry atmosphere of her office, so the patient was motivated to try them.
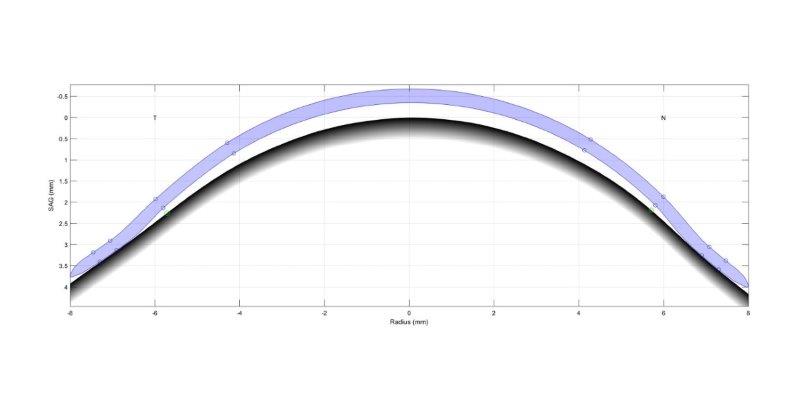
Fig 3. Schematic of lens profile on eye
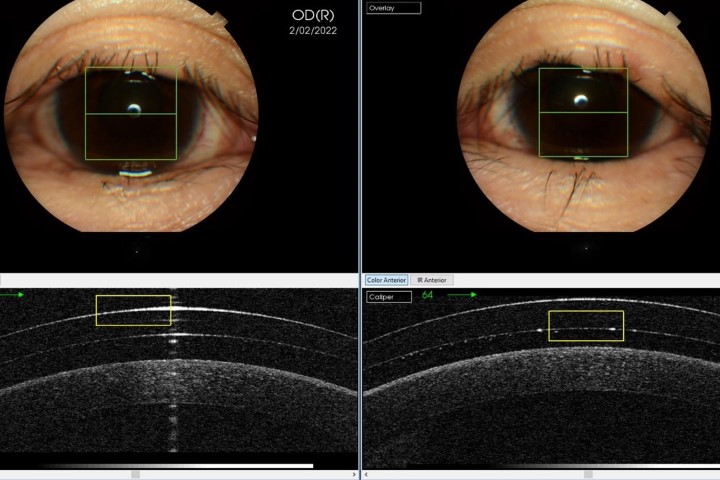
Initial maps were taken and used to design the lenses (Fig 1-3). At the patient’s aftercare appointment she was asked to wear the lenses for at least three hours (images of the lens on the eye and OCT scans are shown in Figs 4 to 7). OCT scanning is very useful in assessing post-wear fits as it allows for effective measurement of lens clearance at the apex and at the limbus, and for accurate assessment of the edge profile and its interaction with the sclera.
![]()
Fig 5. Anterior OCT scan after 3 hours of lens wear showing adequate central clearance
![]()
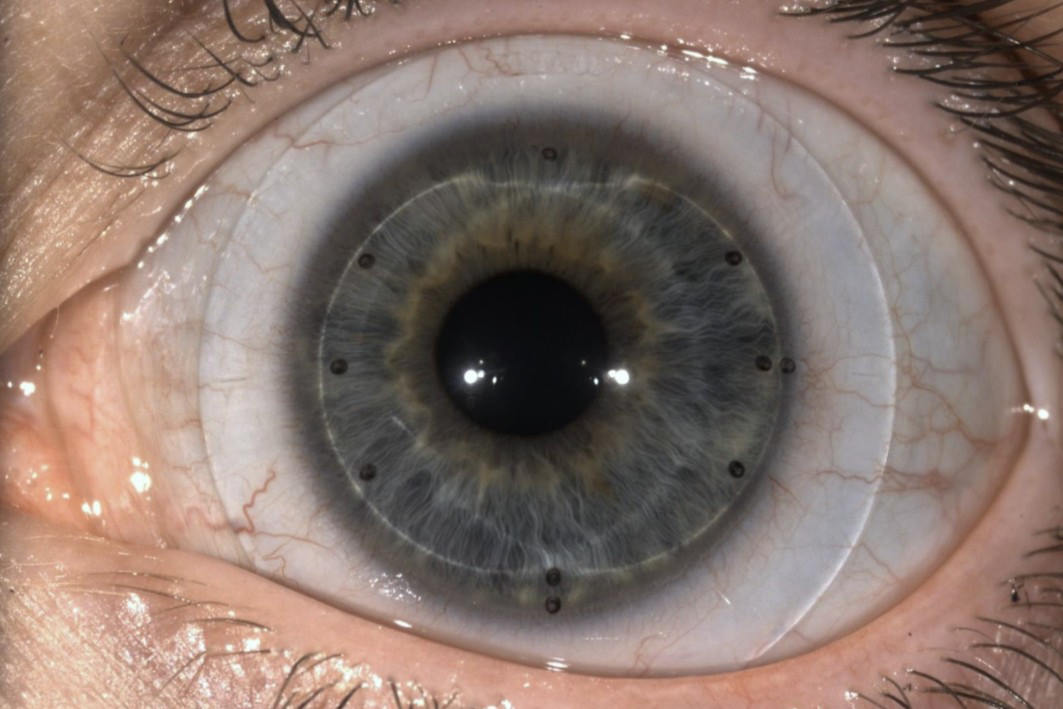
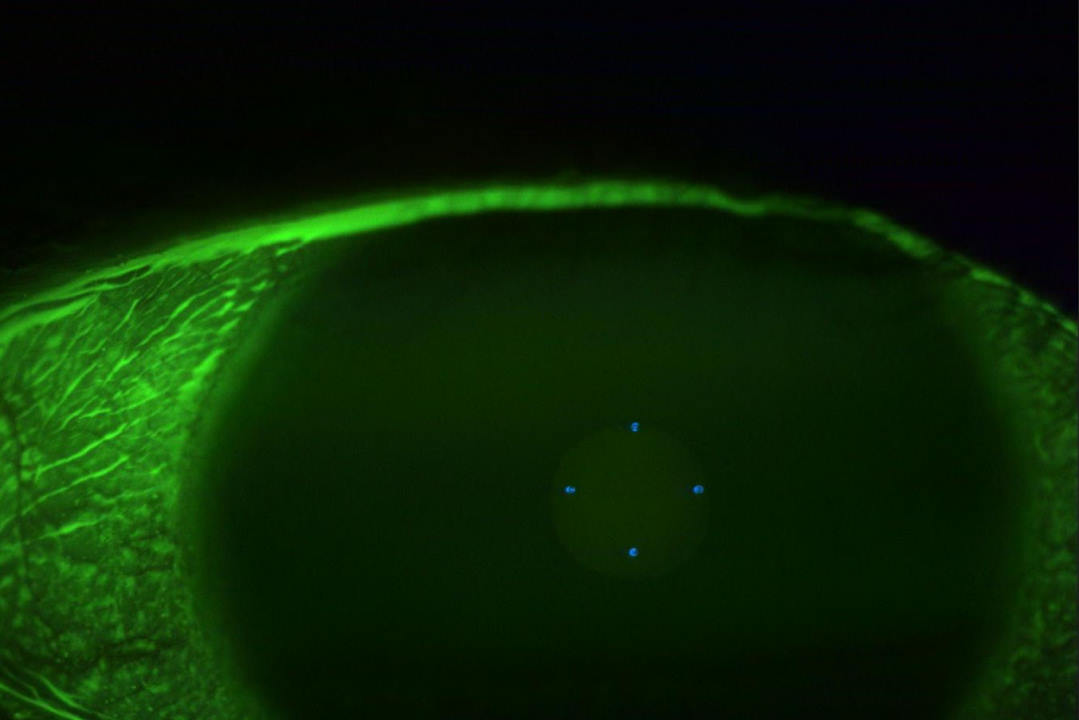
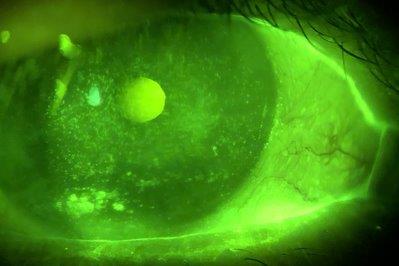
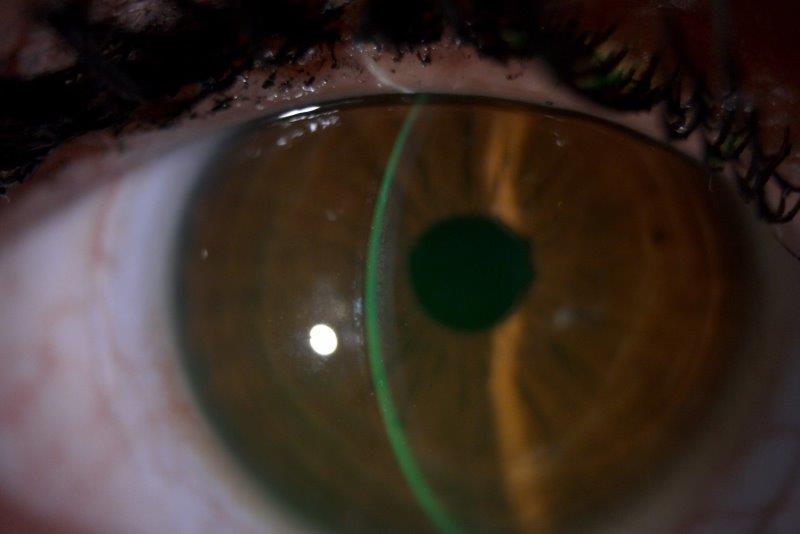
Fig 6. Lens on eye with NaFl in tear film showing adequate clearance centrally and at limbus. Note rotation mark at 6 o’clock
![]()
Fig 7. Anterior OCT scan after 3 hours of lens wear showing adequate medial limbal clearance and customised edge profile that follows the contours of the sclera
The patient doesn’t need to wear the lenses at home but she has worn them for her entire workday and reports being comfortable and better able to tolerate her dry work environment.
Conclusion
With the sMap3D I have found that it is much easier to get the lens fit right from the first attempt, compared with diagnostic fitting, reducing my chair time by 80-90%. This time saving has been passed on to patients as a reduction in fitting fees and it creates a more pleasant experience for the patient, allowing me to offer scleral lenses to more patients. I can now fit more dry eye patients with scleral lenses when they are needed, increasing the scope of both my dry eye and contact lens practice.
References
1. Michaud L et al, The official guide to scleral lens terminology. Contact Lens and Anterior Eye, 2020. 43(6): p. 529-534.
2. Nguyen MT, Thakrar V and Chan CC, EyePrintPRO therapeutic scleral contact lens: indications and outcomes. Canadian Journal of Ophthalmology, 2018. 53(1): p. 66-70.
3. Woods CA, Efron N and Morgan P, Are eyecare practitioners fitting scleral contact lenses? Clinical and Experimental Optometry, 2020. 103(4): p. 449-453.
4. Shorter E et al, Keratoconus patient satisfaction and care burden with corneal gas-permeable and scleral lenses. Optometry and Vision Science, 2020. 97(9): p. 790-796.
5. Kreps EO et al, Mini-scleral lenses improve vision-related quality of life in keratoconus. Cornea, 2021. 40(7): p. 859-864.
6. Bavinger JC, DeLoss K and Mian SI, Scleral lens use in dry eye syndrome. Current opinion in ophthalmology, 2015. 26(4): p. 319-324.
7. Jones L et al, TFOS DEWS II Management and Therapy Report. Ocul Surf, 2017. 15(3): p. 575-628.

Ryan Mahmoud is a therapeutically trained optometrist and owner of NVision Eyecare in Auckland, New Zealand. NVision offers speciality services in myopia control, RGP contact lens fitting and dry eye. Disclaimer: Ryan Mahmoud has no financial interest in the sMap3D.