The 2025 Specsavers Clinical Conference (SCC2025) was a glitteringly green affair, attracting nearly 1,000 optometrists from across Australia and New Zealand, from inside and outside Specsavers, to the Grand Hyatt Melbourne.
Themed ‘Sharpen your focus’, the annual event included: two days of 40-minute CPD sessions presented by some of the region’s leading specialists; the winners’ announcement for this year’s Doug Perkins Medal and Dame Mary Perkins Awards; an evening of cocktails and networking; practical workshops on low-level light therapy; fringe talks from exhibitors; and an additional on-demand programme covering issues from ‘dementia-friendly eyecare’ to ‘retinal red flags’.

SCC2025’s Saturday night entertainment at The Residence, Grand Hyatt Melbourne
The in-person event was hosted by clinical services development consultant Tina Ngan, who kept the sessions impressively to time, while the opening address was given by one of Specsavers ANZ’s best-known personalities, clinical services director Dr Ben Ashby.
Since rolling out its ‘Avoidable Blindness’ programme in 2009, Specsavers has helped reduce avoidable blindness by 94% in the region, donated more than AU$11 million to Fred Hollows through its community programme and helped register more than 240,000 Australians with diabetes for regular eye-check reminders, reported Dr Ashby. It has also recycled more than 20 tonnes of optical waste since partnering with Opticycle in mid-2023, he said. Noting the huge increase in glaucoma detection rates since OCTs were rolled out across the group in 2020, with more than 170,000 glaucoma patients identified to date, special mentions were given to Specsavers Masterton and Batemans Bay, NSW, for their work in this area. Dry eye, contact lenses and kids were other key growth areas, said Dr Ashby, especially myopia management (with Specsavers Onehunga and Hurstville, NSW, getting special mentions). Sticking with kids, more materials featuring Specsavers kid-friendly ‘Optomonsters’, including lollies, stickers and colouring supplies, as well as booster seats for optometry chairs, are being rolled out across the network, he said.
Glaucoma and neuro-ophthalmology to inflammatory eye diseases
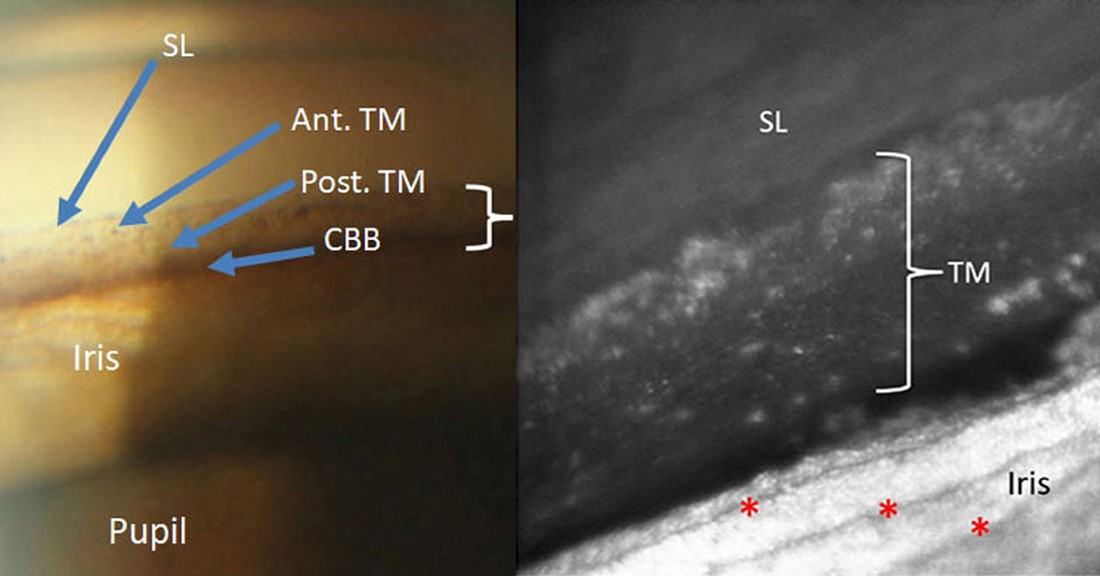
The formal education sessions kicked off with an in-depth look at optical coherence tomography (OCT) and visual field test results in glaucoma. Sydney Eye Hospital’s Dr Jason Cheng shared what he looked for when piecing together glaucoma’s visual clues. OCT is “very good” at detecting glaucoma, he said, but it’s not definitive on its own. Clinical context, history and correlation with the Humphrey Visual Field test and intraocular pressure measurements are important to provide a full picture to identify the presence of glaucoma and monitor progression, he said.

Hector Leong, Youssef Elebiary, Hayden Lee and Woo-Sung Jeh
Melbourne-based glaucoma specialist Dr Tu Tran then discussed glaucoma management, risk assessment and collaborative care, using a series of illustrative cases. She highlighted the key findings of the Laser in Glaucoma and Ocular Hypertension (LiGHT) Trial, which showed that selective laser trabeculoplasty, together with drops, was an effective management strategy for most glaucoma patients.
Fellow Melburnian, neuro ophthalmologist Dr Kate Reid provided a practical take on assessing the urgency of an idiopathic intracranial hypertension (IIH) presentation. Stereotypical IIH patients are obese women of child-bearing age; all others are not stereotypical so need to be assessed carefully, as papilloedema, a key sign of IIH, can also result from other more life-threatening conditions, such as brain tumours or meningitis.

Neuro-ophthalmologist Dr Kate Reid presenting on IIH
The 30-2 visual field test most accurately triages the degree of visual threat in IIH and weight loss, derived from GLP-1 receptor agonists (such as Ozempic or Wegovy), of 5–10% can significantly improve IIH symptoms. These new weight-loss drugs do have significant side effects, however, said Dr Reid, especially muscle loss and non-arteritic anterior ischaemic optic neuropathy.
In a related talk, Vision Eye Institute’s Dr Rushmia Karim presented ‘Anisocoria to headaches – to fear or not to fear’, again using a series of cases. She demonstrated differences between harmless physiologic anisocoria and pathologic anisocoria, which could indicate Horner syndrome, third-nerve palsy, giant cell arteritis or multiple sclerosis. Pathological anisocoria can also be caused by antidepressants, motion sickness patches or even some glaucoma eye drops, she said, so a taking a detailed history, as well as undertaking a comprehensive eye exam, is essential.

Linde Augenstein, Sean Mahendran and Philip Walsh
Saturday afternoon focused on uveitis and eyelid lesions. Associate Professor Mei-Ling Tay-Kearney from the Lions Eye Institute and Royal Perth Hospital tackled anterior uveitis and ‘When to think outside the box’, while Sydney’s Associate Professor Elisa Cornish navigated ‘Through the haze of posterior uveitis’.
With anterior uveitis, it’s always important to examine the back of the eye to make sure it’s not posterior or panuveitis or an infection, said A/Prof Tay-Kearney. But for posterior uveitis, if there are cells in the anterior chamber always confirm it’s not acute retinal necrosis first, said A/Prof Cornish. If you’re not sure, check the patient the next day, she said, noting that posterior uveitis patients always require a lot of time to take a comprehensive history and often collaboration with other health specialists.

Specsavers ANZ’s marketing and SCC2025 events team and presenters with hosts Dr Ben Ashby and Tina Ngan (standing, centre)
Queensland-based Dr Ebony Smith ended the day with a fascinating and very practical look at eyelid lesions and when these should be referred urgently. Key differences between benign and potentially malignant eye lesions are that the latter can include a loss of lashes, ulceration (bleeding, crusting) and infiltration (spreading, colour and shape changes), while benign lesions often have hair, are slow growing and can look ‘stuck on’, she said.
From kids to anterior and posterior eye diseases
Sunday morning focused on paediatric eyecare. Using a series of real cases, Christchurch-based paediatric ophthalmologist Dr Liz Conner covered sore red eyes, ‘funny’ optic nerves, double vision and how to get the best out of younger patients and their parents. Beware conjunctivitis isn’t something more serious, she said, which is likely if it’s unresponsive to antibiotics, there’s no discharge, the child’s had recurrent episodes or their behaviour is affected by their symptoms. Using cases to detail different diagnoses and management strategies for different types of keratoconjunctivitis patients, she also noted that allergic eye disease, though common, can be severe and eye rubbing is not benign, as it can lead to keratoconus. Sudden onset diplopia is always a red flag, she added, especially if associated with headaches, lethargy or fevers as it can be a sign of stroke, aneurysm, cranial nerve palsies or a brain tumour.

Jessica Chen, Sonia Lu and Livia Lai
It pays to take time with paediatric patients to take a thorough history and conduct a detailed eye exam, including OCT, and not jump to any conclusions when a parent says their child can’t see well, said Dr Conner, as it’s easy to miss some serious eye diseases. Slow down, she said, use appropriate language and listen when you’re dealing with kids and if you have any concerns refer immediately to a paediatric ophthalmologist.
Well-known Australian myopia specialist Dr Kate Gifford provided a practical overview of myopia management, from starting the conversation to selecting the right treatment plan. A handy ‘Managing myopia guidelines’ infographic can be downloaded in 20 languages, together with a number of other free resources from her website.

Specsavers’ clinical services director Dr Ben Ashby with speakers Drs Kate Gifford and Liz Conner
Sydney University’s Professor Chameen Samarawickrama, then tackled corneal ulcers through a series of hypothetical cases, cleverly using AI to transform himself into a young then an old woman patient, causing much mirth among the audience. Always assume the most probable and the worst-case scenario (microbial keratitis), treat to cover both, refer quickly and ensure you follow up very closely, he said.
Sydney medical retina specialists Associate Professor Samantha Fraser-Bell and Dr Tuan Tran presented the last two sessions of the conference focusing on geographic atrophy (GA) and retinal care. The limited treatments now available for GA work best the earlier GA is detected, said A/Prof Fraser-Bell, but they do not restore vision, so patient monitoring and counselling is essential, especially to reduce environmental risk factors to slow GA onset.