Uveitis makes up a significant proportion of acute presentations to optometry and ophthalmology clinics. The task of evaluating an undifferentiated uveitis patient can be intimidating. Fortunately, modern imaging technologies help with their diagnosis, treatment and monitoring. Multimodal imaging has also helped enhance our understanding of disease pathophysiology in many uveitic conditions. The imaging tools valuable in uveitis include optical coherence tomography (OCT), ultra-widefield fundus imaging, fundus autofluorescence, fluorescein angiogram and indocyanine green angiogram. Here, we discuss the clinical applications of each of these imaging modalities, with examples to illustrate their role in uveitis management.
Optical coherence tomography
OCT is widely available and used for the detection and monitoring of macular pathology. In uveitis, its main role has been in the detection and monitoring of sequelae of ocular inflammation, including cystoid macular oedema, epiretinal membrane and choroidal neovascular membrane. OCT can frequently obtain images of macular structures, even in the presence of small pupils or media opacity where clinical examination is limited.
OCT is an important diagnostic tool in uveitis because it allows cross-sectional visualisation of the layers of the retina affected by the disease. It can help establish the likely cause of retinitis and aid treatment decisions while awaiting laboratory testing. For example, in toxoplasma chorioretinitis (Fig 1A), OCT over the lesion will typically show full-thickness disruption of the retina with thickening of the choroid. In contrast, viral retinitis (herpes simplex virus, varicella zoster virus and cytomegalovirus) causes full-thickness retinal inflammation but usually spares the choroid1. Syphilis-related posterior uveitis can present with a range of inner and outer retinal changes on OCT2.
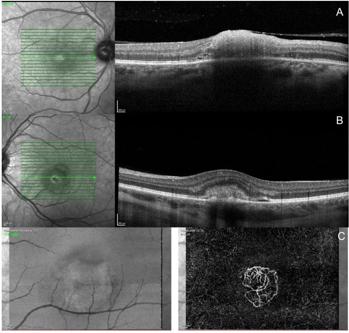
Fig 1. OCT. A) Toxoplasma chorioretinitis involving the macula. B) inflammatory choroidal neovascular membrane in PIC. C) the CNVM visible in 1B demonstrated on OCT angiogram
Enhanced depth imaging (EDI), a modified OCT, allows better imaging of the choroid and sclera and is particularly useful in evaluating choroidal disease. It enables measurement of choroidal thickness, visualisation of the choroidal vasculature and detection of choroidal masses such as choroidal granulomas. EDI-OCT is most useful in uveitic conditions involving the choroid, such as sarcoidosis, Vogt-Koyanagi-Harada syndrome (VKH) and birdshot chorioretinopathy. A thickened choroid with undulations will support a diagnosis of VKH (in a patient with compatible history and examination features) and can be used to monitor recovery as well as early suggestion of relapse3.
OCT angiography
A more recent addition to OCT technology is OCT angiography (OCT-A). This is a non-invasive and quick method of detecting choroidal neovascular membranes (CNVM), which is particularly helpful when fundus fluorescein angiogram (FFA) is not easily accessible or best avoided (eg, in pregnancy). For example, in patients with punctate inner choroidopathy (PIC) (Fig 1B, C) or multifocal choroiditis (MFC), OCT-A is useful for picking up a subtle secondary inflammatory CNVM and differentiating it from a flare of choroiditis. OCT-A has also helped our understanding of some uveitic entities, for example, in acute posterior multifocal placoid pigment epitheliopathy (APMPPE) it demonstrates decreased blood flow at the level of choriocapillaris, suggesting that ischaemic vasculitis is important in the pathophysiology4.
Ultra-widefield fundus imaging
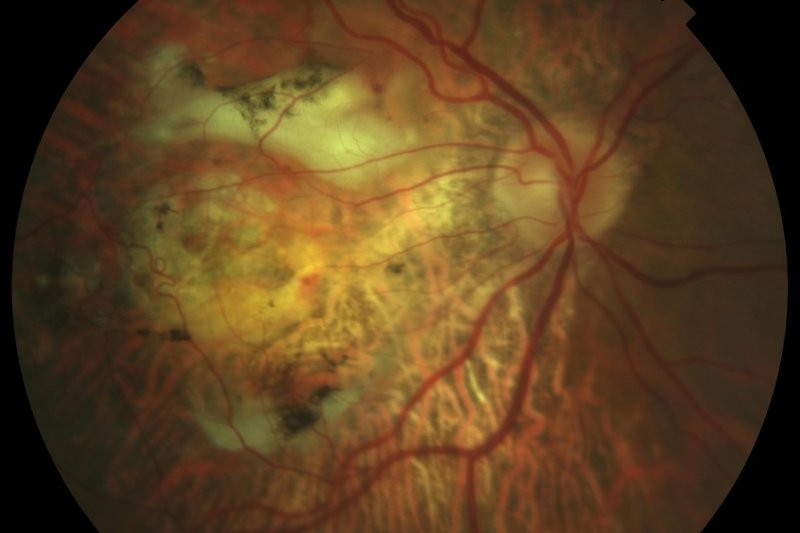
The introduction of ultra-widefield (UWF) fundus imaging has significantly improved the ease of diagnosis and monitoring of retinal pathology. An example is the Optos UWF system which uses confocal scanning laser ophthalmoscopy to produce pseudo-colour digital images of up to 200 degrees of the retina (Fig 2). UWF is very useful in patients with poor dilation from posterior synechiae, media opacity from vitritis and those with peripheral vascular abnormalities which are difficult to see on the slit lamp. Subtle retinal vasculitis can be easily missed on clinical examination, but is easier to identify and monitor on Optos images.
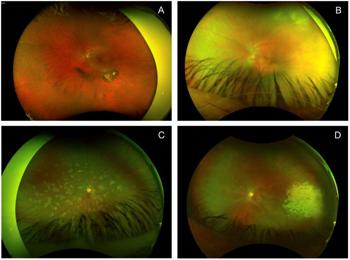
Fig 2. Ultra-widefield imaging. A) Reactivation of toxoplasma chorioretinitis adjacent to an old chorioretinal scar. B) Syphilis-related placoid chorioretinitis. C) Ampiginous chorioretinopathy. D) CMV retinitis with associated vasculitis
Fundus autofluorescence, fluorescein angiogram and indocyanine green angiograms can also be performed on the Optos, providing wide peripheral views to identify pathology otherwise not captured. In addition, some UWF systems can also incorporate image-guided OCT and allow OCT scanning through a peripheral lesion identified on UWF fundus imaging.
Fundus autofluorescence
Fundus autofluorescence (FAF) utilises the fluorescent property of lipofuscin pigments found in retinal pigment epithelium (RPE) and photoreceptor outer segments (Fig 3). The image produced by the emission signal of excited lipofuscin reflects the health of the RPE and outer retina. Hyper-autofluorescence occurs as a result of RPE dysfunction, while hypo-autofluorescence is found where there is RPE atrophy.
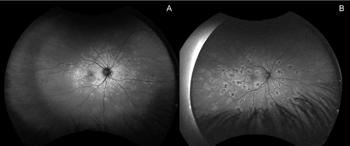
Fig 3. Fundus autofluorescence. A) MEWDS. B) FAF of the same patient in Fig 2C, with ampiginous chorioretinopathy
A group of conditions for which FAF is particularly useful is the ‘white dot syndromes’, including multiple evanescent white dot syndrome (MEWDS) and acute zonal occult outer retinopathy (AZOOR). The fundus examination in MEWDS can be unremarkable early on, but FAF will show characteristic wreath-like hyper-autofluorescent lesions around the optic nerve and macula. This has helped establish the pathophysiology of MEWDS as probable inflammation of the photoreceptors. AZOOR has a characteristic trizonal pattern of autofluorescence on FAF5. These conditions are best evaluated with multimodal imaging, as characteristic patterns on each test contribute to the diagnosis.
Fundus fluorescein angiogram
FFA remains a valuable tool in the assessment of patients with intermediate, posterior and panuveitis and retinal vasculitis. Fluorescein sodium solution is injected into a peripheral vein and serial fundus images are taken to observe the movement of dye through the retinal vascular system. The small unbound fluorescein molecules leak from inflamed retinal vessels due to breakdown of the blood retinal barrier, thus FFA can differentiate between active and inactive disease and also monitor the degree of activity.
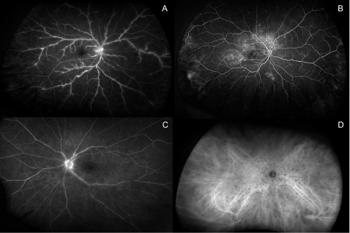
Fig 4. Retinal angiography. A) FFA of tuberculosis-related retinal vasculitis. B) FFA of VKH syndrome. C) FFA of retinal vasculitis in birdshot chorioretinopathy. D) ICGA showing ‘birdshot lesions’ in birdshot chorioretinopathy
FFA is used to look for cystoid macular oedema (CMO), CNVM, retinal vasculitis, retinal ischaemia, as well as neovascularisation (Fig 4). This is in contrast to OCT angiography, which can show areas of non-perfusion or structural change, but cannot show vascular leak, inflammation or other markers of vessel function. FFA is frequently performed in patients with infectious and non-infectious intermediate and posterior uveitis and retinal vasculitis. In occlusive retinal vasculitis, FFA is used to guide targeted retinal photocoagulation to treat secondary neovascular complications.
Indocyanine green angiogram
Indocyanine green angiogram (ICGA) complements FFA but focuses on the choroidal circulation as opposed to the retinal vasculature. The indocyanine green molecules are 98% protein bound and do not readily pass through the fenestrations in the choriocapillaris, thus allowing better visualisation of the choroidal vasculature. ICGA is useful in inflammatory conditions involving the choroid including sarcoidosis, VKH and birdshot chorioretinopathy. It is particularly important in the diagnosis of birdshot chorioretinopathy because birdshot lesions are clinically very subtle and easily missed early on, but are numerous and obvious on ICGA. Birdshot chorioretinopathy will also commonly show widespread vascular leak on FFA. In VKH, ICGA is used for monitoring disease activity and response to treatment. The choroidal granulomas in active VKH appear as hypofluorescent dark dots (HDDs) on ICGA6. Treatment is aimed at resolution of these HDDs. A normal ICGA excludes choroidal involvement and helps to narrow down the differential diagnosis in cases of undifferentiated uveitis or retinal vasculitis.
Conclusion
Multimodal imaging has an important role in the diagnosis, treatment and monitoring of patients with uveitis. Understanding the indications for each imaging modality and the correct interpretation of findings will improve diagnostic accuracy, guide the correct treatment plan and improve patient outcomes.
References

Dr Lucy Lu is a senior uveitis fellow at the University of Auckland and Greenlane Clinical Centre.

Dr Jo Sims is a medical retina and uveitis specialist at Eyes and Eyelids and Greenlane Clinical Centre in Auckland. She is a trustee for Macular Degeneration NZ and is on the Pharmac Ophthalmology Subcommittee.