




Glaucoma management has traditionally been focused on medical therapy as initial treatment with intensification until maximum tolerated medical therapy (MTMT) is reached. Often patients end up taking multiple eyedrops several times a day, which can sometimes lead to issues with side effects and adverse events, poor adherence, inconvenience and reduction in quality-of-life measures.
The results from the ‘Laser in glaucoma and ocular hypertension trial’ (LiGHT) indicated that selective laser trabeculoplasty (SLT) may offer better glaucoma control over medical therapy in the initial treatment of primary open-angle glaucoma (POAG) and ocular hypertension (OHT)1. The development of safer and less invasive surgical options, termed minimally invasive glaucoma surgery (MIGS) has enabled surgical intervention at an earlier stage as an alternative to intensive medical therapy.
Although medical treatment still remains an important part of glaucoma care, these newer developments are leading to a paradigm shift in glaucoma management, where we are able to offer patients safe and effective alternatives if they are struggling with multiple daily eyedrop usage. Many MIGS procedures are now readily available for clinical use in New Zealand and have become an essential part of our current glaucoma management armamentarium.
MIGS
MIGS refers to a group of newer glaucoma procedures considered less invasive in comparison to traditional glaucoma surgery, while still providing meaningful intraocular pressure (IOP) lowering. They have been developed to bridge the gap between initial medical and SLT treatment and the more invasive options of trabeculectomy and tube-shunt surgery. The different MIGS procedures share common characteristics, including a high safety profile, minimal disruption of normal anatomical structures, ease of use and rapid recovery time. MIGS may be combined with cataract surgery or be performed as standalone procedures.
MIGS procedures have been developed to target almost every aspect of both the conventional and uveoscleral aqueous outflow pathways. The most common MIGS devices currently used in New Zealand include the iStent (Glaukos),, Kahook Dual Blade (KDB, New World Medical) and the Preserflo MicroShunt (Santen).
iStent
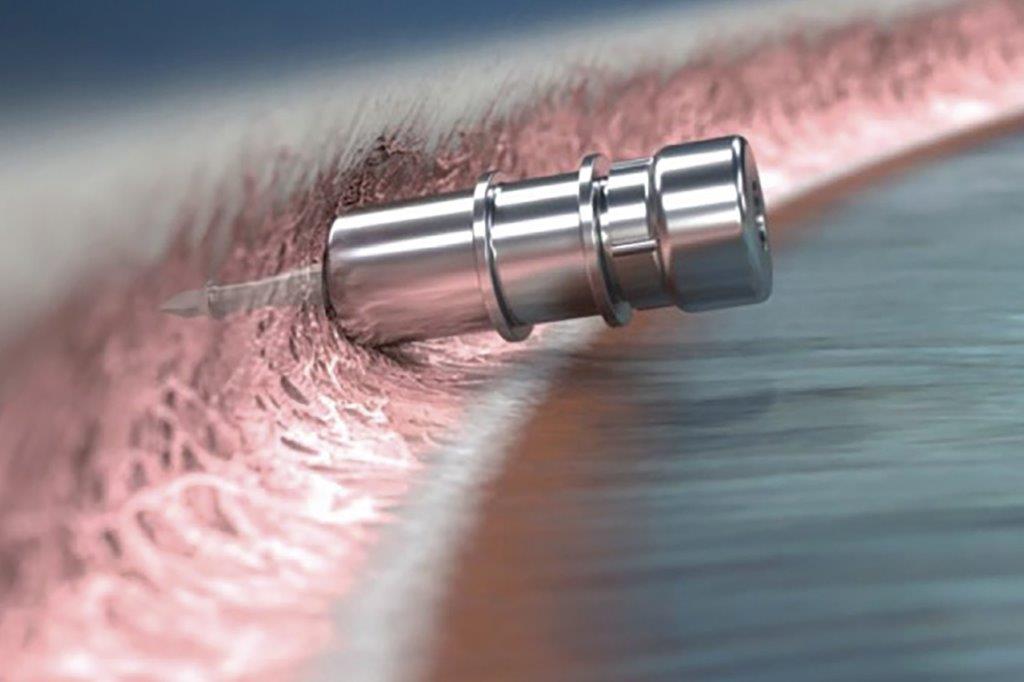
iStent is a MIGS device implanted into the trabecular meshwork (TM) to enable drainage of aqueous humour from the anterior chamber directly into Schlemm’s canal, bypassing the TM (Fig 1). It’s recommended for patients with mild to moderate POAG, OHT, normal-tension glaucoma (NTG), pseudoexfoliative glaucoma (PXG) and pigmentary glaucoma (PG). iStent is contraindicated in patients with angle-closure glaucoma and most forms of secondary glaucoma other than PXG/PG. As the iStent is most commonly used in combination with cataract surgery, the patients most suitable would be those who also have visually significant cataract along with being on multiple glaucoma eye drops and/or having uncontrolled glaucoma.

Fig 1. The iStent inject
The safety and efficacy of iStent is now well established. Meta-analysis data confirms the superiority of iStent with cataract surgery over cataract surgery alone, in terms of both absolute IOP lowering and number of medications needed for glaucoma control2. The clinical benefits are often sustained for many years post-operatively2. The current generation of iStent (iStent inject W) allows for two devices to be injected into the TM of the same eye using a single pre-loaded injector. A recent prospective randomised multi-surgeon trial demonstrated that with the use of two iStent injects in the same eye, it is also safe and effective as a stand-alone procedure (without cataract surgery) for the treatment of mild to moderate glaucoma3.
iStent technology has progressed further with the introduction of the iStent infinite, which enables three iStents to be injected into the TM with the same injector. Research has shown this leads to additional IOP lowering and better glaucoma control than what was achieved with two iStents4. This could potentially play a role in patients with more advanced glaucoma and evidence suggests it may be effective even in patients with previous failed glaucoma surgery4.
KDB
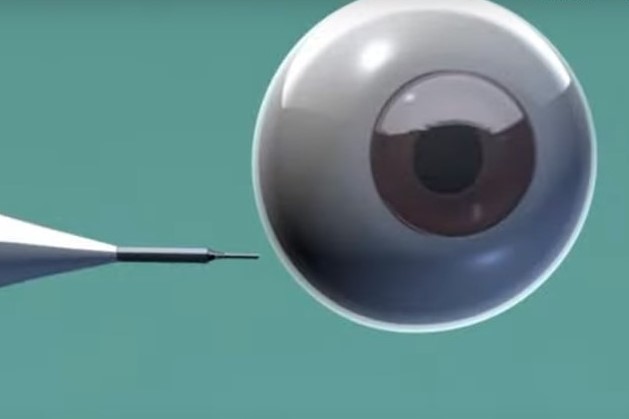
The KDB is another MIGS procedure targeting the TM and would be considered an alternative to iStent. The KDB is a specifically designed goniotomy blade that allows the ab interno (via anterior chamber) removal of a strip of TM while minimising collateral damage to surrounding structures (Fig 2). By removing a section of TM, the KDB allows aqueous drainage directly into the collector channels of Schlemm’s canal and the distal outflow system. KDB can be performed as a standalone procedure or combined with cataract surgery. Similar to iStent, the ideal patient has mild to moderate open-angle glaucoma, is on multiple medications and undergoing cataract surgery.

Fig 2. Kahook Dual Blade goniotomy
Clinical studies have demonstrated a high safety profile comparable to other MIGS procedures and enhanced safety when compared to trabeculectomy5. The clinical efficacy, in terms of long-term IOP lowering and reduction in number of medications, is also comparable to other MIGS procedures5. KDB may be effective in severe or refractory glaucoma and hence the iStent infinite could provide a possible alternative in high-risk eyes that would otherwise need more invasive surgery6.
Preserflo MicroShunt
The Preserflo MicroShunt can be considered the next level in MIGS intervention when iStent or KDB is unsuitable or unsuccessful for a particular patient. The Preserflo device provides greater IOP lowering than these other MIGS devices and is best suited to patients with uncontrolled moderate to advanced glaucoma. Preserflo is considered a more direct alternative to trabeculectomy than other MIGS procedures.
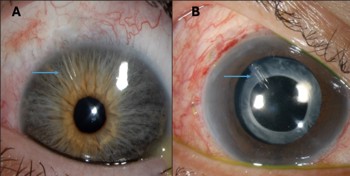
Fig 3. The Preserflo MicroShunt (A) in comparison to a traditional tube-shunt (Paul tube in the sulcus) (B)
The device is a ‘microtube’ made from biocompatible material known as ‘SIBS’ (synthetic polymer of poly(styrene-block-isobutylene-block-styrene)) and is 8.5mm long with a 350mm outer diameter and 70mm lumen. These dimensions were designed to allow adequate outflow while preventing hypotony. The Preserflo is implanted subconjunctivally through a scleral tunnel so that the proximal tip rests in the anterior chamber and the distal end sits under the conjunctiva and the Tenon capsule approximately 6mm from the limbus (Fig 3A). Aqueous drains from the anterior chamber to the subconjunctival space, resulting in the formation of a bleb much like with a trabeculectomy – hence mitomycin-C application within the sub-conjunctival space at the time of surgery is required. Unlike trabeculectomy, there is no need for scleral flap formation, sclerotomy or iridectomy as part of the procedure.
Preserflo requires less operating time and post-operative additional measures, has a faster recovery time and a lower risk of intraoperative and post-operative complications, compared to trabeculectomy7-9. Several clinical trials evaluating Preserflo have demonstrated a high safety profile and effectiveness at controlling glaucoma over many years of follow up7-9. The complete success rate (no additional medications to achieve target IOP) was reported to be between 75–80% and the qualified success rate (requiring additional medications) was over 90% in these studies at least two years after surgery. However, Preserflo does not result in the same level of IOP lowering that can be achieved with trabeculectomy, hence for patients who require a low target IOP, the latter option is still preferred9.
The current role of trabeculectomy and tube-shunt surgery
With the advent of MIGS there has been a decreasing trend in the need for trabeculectomy. However, it has long been considered the gold standard of glaucoma surgery and still has an important role to play. Trabeculectomy is the preferred option in patients with uncontrolled moderate to advanced glaucoma on MTMT who require a low target IOP. Furthermore, trabeculectomy may be necessary when access to MIGS is not possible or as a subsequent step if previous MIGS was unsuccessful.
Traditional tube-shunt surgery (Ahmed, Baerveldt, Molteno and Paul implants) will also continue to play an essential role due to their different clinical indications. In particular, patients with complex secondary glaucoma (eg, active neovascular or uveitic glaucoma) have far better outcomes with tube-shunt surgery than with trabeculectomy. Other indications include conjunctival scarring precluding filtration surgery or previous failed trabeculectomy.
In contrast to Preserflo, these tubes have a much larger lumen diameter and an external plate implanted subconjunctivally, which allows for formation of an external reservoir. Tube-shunts are available in different sizes, material and design, with some being valved and others non-valved. The Paul tube (Fig 3b) is a relatively new device with a lumen diameter (0.1mm) somewhat midway between the Preserflo (70mm) and other tubes (0.3mm) and has been well-adopted as it maintains the clinical effectiveness of other tube-shunts while having a lower risk of hypotony and other post-operative complications.
References

Dr Hussain Patel is a glaucoma and cataract specialist at Eye Surgery Associates and Greenlane Clinical Centre in Auckland. He is also a senior lecturer with the Department of Ophthalmology, University of Auckland.