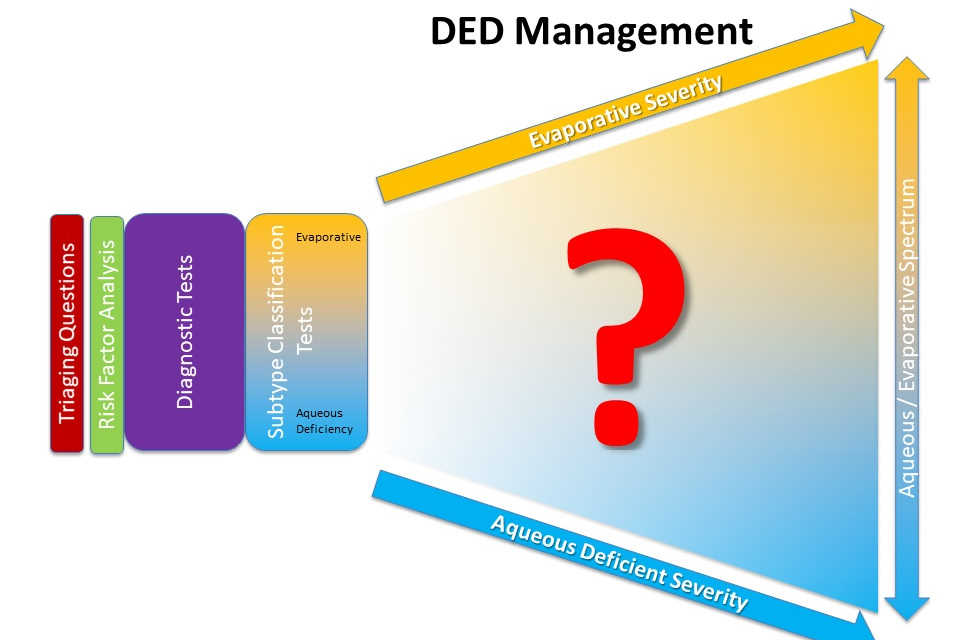
The TFOS DEWS II reports were published in 2017, bringing practitioners up to date on the scientific evidence related to dry eye disease (DED), including our current understanding of its pathophysiology, a consensus-refined definition, a more definitive approach to diagnosis and a review of management options. However, it also identified a lack of randomised clinical trials that are important for informing practitioners about relative efficacy of available management options at different levels of disease severity and across the subclassification spectrum, from evaporative to aqueous deficiency.
As a starting point in addressing this gap in knowledge, a cross-sectional study was designed to establish current practice norms. An anonymous online questionnaire was distributed to eye care professionals around the world. Translated into 14 different languages, this six-question survey sought to determine the management and treatment approaches used by eye care practitioners (ECPs) worldwide, based on disease severity and subclassification.
The survey was completed by 1,139 eyecare professionals (37% ophthalmologists and 58% optometrists) from 51 countries. It identified that management varied significantly by continent and by country (p<0.01). Globally, 83% of practitioners reported offering their patients advice, irrespective of DED subtype, about environment, diet and hydration.
Practitioners treating DED across all severity levels prescribed some treatments largely independently of severity, such as artificial tears (~80%) and essential fatty acids (~45%); they prescribed other therapies similarly for both moderate and severe forms of the disease, including in-office lid management (29-57%) and topical antibiotics (8-35%); while they were observed to prescribe other treatments, such as oral antibiotics (4-43%) and punctal plugs (5-48%), predominantly in patients with severe disease.
The most frequently prescribed treatments for aqueous deficient DED were artificial tears (88%), punctal plugging (51%) and topical antibiotics (38%), whereas, for evaporative DED, between 50 and 60% of practitioners prescribed essential fatty acids, artificial tears (particularly those containing lipids), lid wipes, hot compresses and/or in-office lid hygiene procedures.
This research revealed that a wide range of management strategies are utilised across different DED severity levels and subtypes. DED management, and the treatments applied, were observed to differ between continents and countries. The survey results are valuable for enabling practitioners to benchmark their current practice against regional and global norms and to help drive research that will best inform clinical practice in the future.
Sonia Trave Huarte and Professor James Wolffsohn are from Aston University, Birmingham, England. Their co-authors on the study include Professor Lyndon Jones, director of the Centre for Ocular Research and Education at the University of Waterloo, Canada, and Associate Professor Jennifer Craig and Dr Michael Wang from the University of Auckland.