Blepharitis is a common, underdiagnosed and often untreated eye affliction which may cause a range of clinical manifestations, including irritated eyelid margins, loss of eyelashes, tear film disruption, ocular discomfort and meibomian gland dysfunction1. Causes can include bacterial, viral, fungal or parasitic overgrowth. Demodex blepharitis is caused by an ectoparasite (living outside of the body), of which there are two species in humans, namely Demodex folliculorum, inhabiting eyelash follicles, and Demodex brevis, inhabiting meibomian glands2. An overgrowth of D. folliculorum leads to demodicosis with the pathognomonic sign – clear gelatinous debris surrounding the base of the eyelashes, termed cylindrical dandruff and often associated with itching along the lid margin.

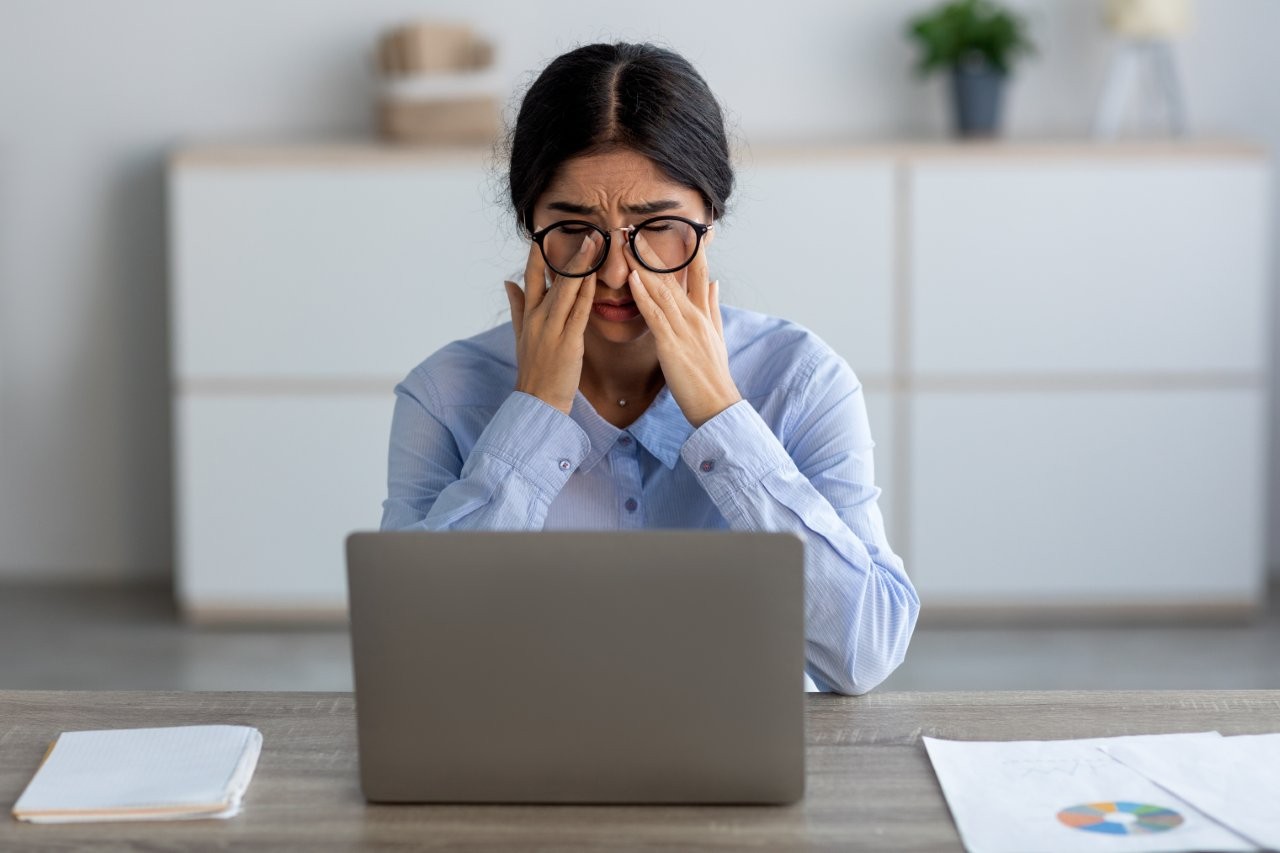
Slit lamp evaluation at 10x magnification showing diffuse collarettes, the waste products of Demodex folliculorum. Credit: Tarsus Pharmaceuticals
The therapeutic strategy is to reduce the quantity of Demodex mites in the lash follicles to ease the bioburden along the lid margin. Traditionally, eyelid hygiene products with tea tree oil (TTO) or one of its derivatives, terpinen-4-ol (T4O) have been recommended to improve symptoms and lower mite counts2. Drawbacks include stinging on the ocular surface and the variability in terms of Demodex eradication3. Additionally, in vitro studies have reported that TTO/T4O are detrimental to meibomian gland epithelial cells4. Other options for management includes intense pulse light therapy (IPL)5, however, this incurs considerable additional expense for patients and requires three to four visits. Further, not all practitioners have access to IPL. Hence, alternative therapeutic treatments for Demodex are needed.
Lotilaner 0.25% eyedrop (Xdemvy, Tarsus Pharmaceuticals) is the first FDA-approved (July 2023) medication for the treatment of Demodex blepharitis with a recommended dosing frequency of twice a day for six weeks6. GABA (gamma-aminobutyric acid)-gated chloride channels, critical in the nervous system function of mites, is blocked by Lotilaner resulting in spastic paralysis of Demodex. It is noteworthy that Lotilaner does not target GABA-chloride channels in humans, reducing the risk of adverse effects. Since its US launch, several studies have reported a favourable efficacy and safety profile, supported by meta-analysis reports7-10.
Lotilaner significantly eradicates mites (p<0.0001) and reduces collarette/cylindrical dandruff (p<0.0001), when compared to vehicle alone7-10. Other ocular parameters such as erythema, overall improvement of symptoms (itching, ocular irritation/inflammation) and mite density, also showed favourable outcomes (p<0.0001) with Lotilaner, over vehicle7, 8. Adverse events are rare and mild (mild burning, redness, blurriness, mild skin irritation, eye discharge, dry eye, conjunctival hyperemia, punctate staining of the cornea, photophobia), with the most common being site instillation pain.
Demodex blepharitis is known to be more common with increasing age and in contact lens wearers reporting discomfort, which may even contribute to contact lens dropouts. For these reasons, education of patients of all ages and contact lens wearers to maintain good lid hygiene and address blepharitis as promptly as possible to avoid undesirable effects is important. Lotilaner 0.25% ophthalmic solution, while not available in New Zealand at the current time, is a promising new therapeutic treatment to look out for, for Demodex blepharitis.
References
1. Amescua G, Akpek E, Farid M, et al. Blepharitis Preferred Practice Pattern(R). Ophthalmology 2019;126:56-93.
2. Bitton E, Aumond S. Demodex and eye disease: a review. Clin Exp Optom 2021;104:285-294.
3. Ngo W, Jones L, Bitton E. Short-term comfort responses associated with the use of eyelid cleansing products to manage demodex folliculorum. Eye Contact Lens 2018;44 Suppl 2:S87-S92.
4. Chen D, Wang J, Sullivan D, et al. Effects of Terpinen-4-ol on meibomian gland epithelial cells in vitro. Cornea 2020;39:1541-1546.
5. Zhang X, Song N, Gong L. Therapeutic effect of intense pulsed light on ocular demodicosis. Curr Eye Res 2019;44:250-256.
6. Syed Y. Lotilaner ophthalmic solution 0.25%: first approval. Drugs 2023;83:1537-1541.
7. Muhammad S, Fareed A, Sohaib Asghar M, et al. Efficacy and safety of Lotilaner ophthalmic solution 0.25% for the treatment of Demodex blepharitis: a meta-analysis of randomised controlled trials. Cont Lens Anterior Eye 2024;47:102148.
8. Awan B, Elsaigh M, Tariq A, et al. A systematic review and meta-analysis of the safety and efficacy of 0.25% Lotilaner ophthalmic solution in the treatment of Demodex blepharitis. Cureus 2024;16:e52664.
9. Abo Zeid M, Elrosasy A, Abbas A, et al. Efficacy and safety of Lotilaner ophthalmic solution 0.25% in the treatment of Demodex blepharitis: a systematic review and meta-analysis. Ocul Immunol Inflamm 2024:1-12.
10. Talha M, Haris Ali M, Fatima E, et al. Efficacy and safety of Lotilaner ophthalmic solution (0.25%) for the treatment of Demodex blepharitis: a grade assessed systematic review and meta-analysis of observational & experimental studies. Am J Ophthalmol 2024;264:8-16.

Professor Etty Bitton is director of the Dry Eye Clinic at the University of Montréal, Canada, a TFOS ambassador and clinical researcher, and was a participant in both the TFOS DEWS II and TFOS Lifestyle Workshops.
Patients having difficulty instilling eyedrops?
The squeezability of ocular lubricant bottles may be a challenging task for older patients with reduced hand grip or pinch strength or those suffering from arthritis. Professor Etty Bitton and Dr Joseph Bouskila investigated the force needed to expel a drop from a variety of different ocular lubricant containers. Dr Kalika Bandamwar, undertaking similar research in Auckland, is now collaborating with Professor Bitton following her sabbatical visit in late 2023, to take the next step in this research area.
If you have any patients over 65 years old with or without hand/finger arthritis who are interested in participating in their next study on pinch strength and the squeezability of ocular lubricants, please contact Dr Kalika Bandamwar at the University of Auckland at kalika.bandamwar@auckland.ac.nz.