The impact of blinking on the quality of the tear film layer has gained significant attention in recent times¹. Normal apposition of the upper and lower lids during a complete blink serves to secrete and spread the meibum adequately over the tear film surface. Any disruption in the normal blink can, therefore, compromise the stability of the tear film layer. The increased use of computers has brought about multiple health concerns, including ocular discomfort. Incomplete and infrequent blinking are key abnormalities associated with computer use and have been associated with dry eye symptoms and signs.
Recent research in the Ocular Surface Laboratory (OSL) evaluated the potential for prescribed blinking exercises in retraining and modifying blink patterns to alleviate dry eye symptoms and improve clinical signs².
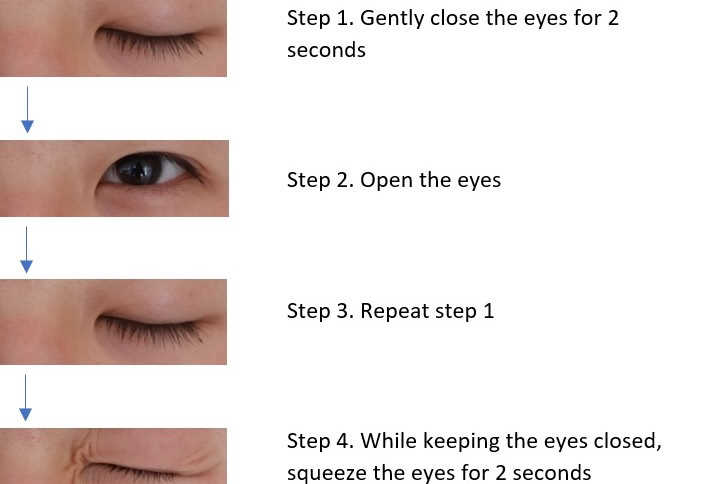
A cohort of 54 participants with dry eye symptoms were recruited and instructed to perform a 10-second cycle of blinking exercises (Fig 1) every 20 minutes during waking hours for four weeks. A total of 41 participants completed the study, reporting an average of 25.6 daily blinking exercise cycles. Improvements in dry eye symptoms were noted on DEQ-5 (11±4 to 7±3; p<0.001) and the OSDI (36±18 to 22±17; p<0.001). Performing daily blinking exercises also resulted in improvements of clinical signs, with increased mean tear film stability (6.5±2.4 to 8.1±4.8 seconds; p<0.04) and fewer incomplete blinks (54±36 compared to 34±29%; p<0.001).
Overall, this pilot study demonstrated that investing in a simple, self-directed blinking exercise routine over just four weeks can significantly improve blink quality as well as signs and symptoms of mild dry eye.
Future research is needed to confirm these benefits across a broader range of disease severity. Meanwhile, blinking exercises may be incorporated in clinical recommendations as an adjunctive therapeutic measure to protect against the impact of digital devices on the evolution of meibomian gland dysfunction and dry eye disease. As with other self-administered therapies, such as warm compress therapy and lid hygiene, patient compliance naturally limits success. Clinicians are encouraged to identify means of increasing patient motivation and therapy adherence.
References
This study was conducted by Dr Andy Kim, as a component of his MBChB selective project at the Unveristy of Auckland, and by honours BOptom student Jason Lee.