Since Alexander Fleming discovered antibiotics in 1928, they have been the major line of defence against bacterial infections. However, over several decades, many antibiotics have gradually lost effectiveness. Given the difficulties associated with developing novel, highly effective antibiotic classes, novel non-antibiotic approaches of managing infections are highly sought after. It’s been a fascinating and exciting journey at the University of Auckland (UoA) over the last decade, being involved in this area, where our work has focused on light-based anti-infective technologies such as UVC light, as well as probiotic-based methods of managing acute infections.
Worldwide, the rise of multidrug-resistant microorganisms has made formerly easily treated infections much harder to manage. Although New Zealand’s population currently has low antimicrobial resistance, this status is fragile due to global migration, growing resistance in other regions and widespread use of antibiotics in the poultry and dairy industries. The global impact is already severe: in 2019, bacterial antimicrobial resistance directly caused an estimated 1.27 million deaths and was indirectly associated with nearly five million. Yet, the rate of discovery of new antibiotic classes has declined significantly. Many promising drugs fail in preclinical and clinical trials, perform poorly against hard-to-kill pathogens, or are abandoned due to high development costs and low governmental investment and limited commercial incentives. International organisations, such as WHO, increasingly emphasise that while antibiotic stewardship is essential, alternative non-antibiotic approaches must now move to the forefront of infection management.
Light, such as UVC, represents a very promising antimicrobial strategy in managing active infections. It is known to act as a natural stressor for microorganisms, including bacteria, fungi and viruses by causing DNA damage, inducing free oxygen radicals, disrupting cytosolic enzymes, crosslinking proteins and damaging cell membranes. Ecological studies suggest microorganisms have evolved over millions of years to tolerate certain levels of natural light, yet there remains a threshold beyond which they cannot survive. The inherent antimicrobial property of light has long been used in applications such as water purification, air disinfection – widely used during the Covid pandemic and in the sterilisation of surgical and medical devices. Attempts in the early 2000s to use UVC light in localised infection management were conceptually sound, but limited clinical data and a lack of well-designed scientific protocols prevented meaningful translation.
Sending in the light infantry
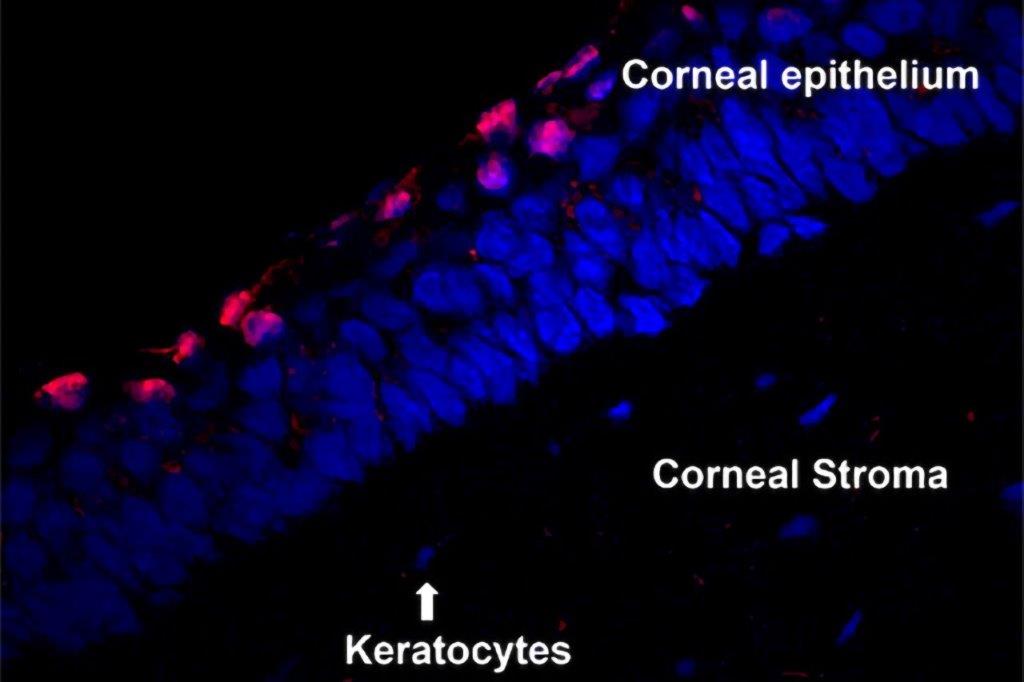
In recent years, our work at the UoA has remained at the cutting edge, leading the field in comprehensive and systematic investigations of UVC in regard to its potential for managing corneal infections. Unlike UVA (the longer-wavelength UV used in corneal collagen crosslinking), UVC is rapidly absorbed by the superficial corneal layers, which avoids interfering with corneal stem cells while exerting strong antimicrobial action at the ocular surface. Study findings have reignited global interest, with several research groups now reporting convergent evidence supporting the safety and efficacy of UVC in managing different infections. Importantly, the New Zealand-based research has progressed to clinical trial, with recruitment for an initial safety and tolerability trial currently underway. Other light-based approaches for managing corneal infections continue to show promise, including antimicrobial blue light and photodynamic therapy. Photodynamic therapy – similar in principle to corneal crosslinking, where UVA activates riboflavin to produce oxygen radicals – has also produced encouraging results, with ongoing innovation in photosensitisers and applied wavelengths.
It is now becoming clear that light-based interventions, such as UVC, could sit among the leading solutions for managing localised infections in the coming decades. Development costs for light-based technologies are lower than for new antimicrobial agents, regulatory pathways are comparatively simpler and improvements in LED technology allow for more precise delivery of narrow wavelength bands to infection sites, with minimal collateral tissue damage and less harm to normal flora compared with antibiotics. As antimicrobial resistance continues to grow, a pragmatic shift toward therapies grounded in physical and biological principles is not desirable but becoming necessary. In an era where antibiotic discovery lags behind microbial evolution, harnessing light would appear to offer a timely, practical and scientifically robust path forward in infection management.
Beyond light-based treatments, some of the most exciting developments are emerging from the use of gut microorganisms (probiotics) in acute infection management. Channelling naturally occurring, harmless microorganisms to inhibit more pathogenic species may offer a powerful and sustainable alternative. Certain probiotic strains can suppress pathogens such as Pseudomonas species by producing their own antimicrobial compounds, highlighting the potential to leverage such interactions rather than relying solely on conventional synthetic drugs. At the UoA, we are expanding this probiotic-focused research to develop novel therapies for more severe corneal infections, aiming to translate them into clinically meaningful solutions. This innovative approach made it through to the finals of the Medicines New Zealand Innovation Jump Start Award 2025.
We warmly welcome anyone interested in antimicrobial research to contribute to taking this research forward, whether through study, collaboration, or any other contribution they can offer. Our goal is to advance antimicrobial research in ocular infection management, building from the strength and innovation of our own communities. While the global challenge of increasing antimicrobial resistance remains, our New Zealand-based efforts have begun taking meaningful steps toward practicable solutions. With more hands and minds joining this work, we believe we can continue shaping a future where effective, locally driven innovation leads the way.
Dr Sanjay Marasini is a senior postdoctoral research fellow in the Department of Ophthalmology at the University of Auckland, and leads a sub-team within the Ocular Surface Laboratory, headed by Professor Jennifer Craig.

Dr Simon Dean is a cataract and oculoplastics specialist working at Re:Vision in private and Manukau Superclinic in Auckland. He is chair of Basic Sciences and COPEM for RANZCO and is active in research, currently working on the potential for UVC to treat corneal infections with his company Photon Therapeutics.