


There was a time when refractive surgery was very much the domain of those surgeons who specifically specialised in excimer laser treatment of the cornea, but rapid advances in corneal refractive surgery techniques and intraocular lens (IOL) technology, as well as greater patient expectations, have brought us to a point where the majority of ophthalmologists who perform cataract surgery can consider themselves refractive surgeons. As an optometrist or ophthalmologist presented with a patient requesting to be spectacle- or contact-lens-free, what options are there and how do we approach them?
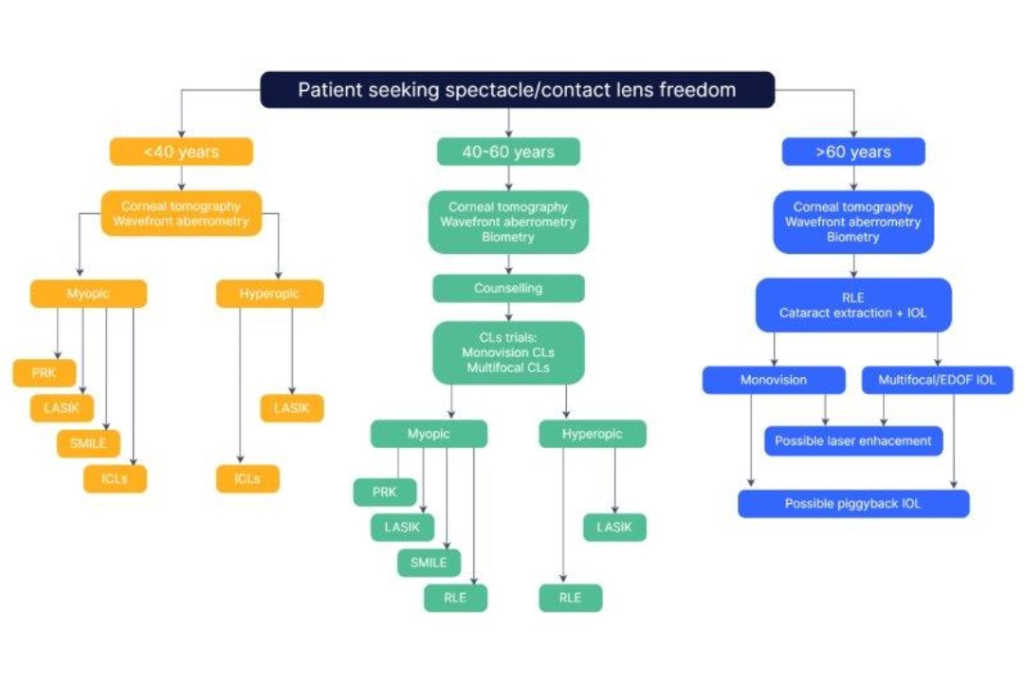
Patients under 40 years old
Patients under 40 years old represent a relatively straightforward group. The vast majority are myopes, although there will be a small number of relatively high hyperopes. Pre-operative refractive stability must be established (which usually means the minimum age for refractive surgery is around 20 years) and to reduce the risk of post-operative keratectasia (iatrogenic keratoconus) all patients require careful pre-operative screening with corneal topography/tomography, as well as an assessment of risk factors, such as eye rubbing and atopy. Dry eye must be assessed and treated vigorously pre-operatively as most laser techniques result in temporary dry eye, particularly in those with pre-existing dry eye.
PRK
Photorefractive keratectomy (PRK) is the original excimer laser treatment, involving removal of the corneal epithelium and precise reshaping of the cornea underneath with an excimer laser. While it results in excellent visual outcomes, it’s a painful procedure to recover from and visual rehabilitation can be slow. Although it has been largely superseded by laser-assisted in situ keratomileusis (LASIK) and small incision lenticule extraction (SMILE), it still represents the safest option for patients with thin corneas.
LASIK
LASIK has been the most commonly performed refractive procedure over the last three decades and modern LASIK techniques result in over 90% of patients achieving uncorrected visual acuity of 6/6 in both eyes, and 99.5% achieving 6/12 or better. Only 0.6% of eyes lose two or more lines of corrected distance visual acuity, and only 1% of patients are dissatisfied with the outcome1. A flap is created in the cornea, historically mechanically with a microkeratome (blade), but now with the use of a femtosecond laser, which significantly reduces the risk of flap complications. An excimer laser then reshapes the cornea underneath and the flap is returned to its original position at the end of the procedure, resulting in much more rapid recovery in terms of both comfort and vision than with PRK.
Contemporary excimer lasers have active eye-tracking systems to compensate for cyclotorsion and microsaccadic movements during the procedure, increasing the accuracy of treatment. The range of treatable refractive error is typically +4D to -10D, with cylindrical correction of 6D, with the degree of treatment limited to that which ensures a minimum residual stromal bed (ie. the amount of cornea that remains untouched) of 250-300μm. Outcomes in some patients may be improved by tailoring the excimer laser ablation pattern to reduce a patient’s natural higher order aberrations (such as coma, trefoil and spherical aberration) as measured by a wavefront aberrometer pre-operatively.
All patients need to be counselled on temporary suboptimal effects such as post-operative glare or halos, plus dry eye, as well as more permanent complications such as reduction of vision from corneal scarring due to diffuse lamellar keratitis, infection, epithelial ingrowth and keratectasia. Dry eye is a relatively common LASIK side effect, albeit usually temporary, but may require management with lubricants, punctal plugs and management of meibomian gland dysfunction.
SMILE
Small incision lenticule extraction (SMILE) is the newest laser treatment, first performed in 2008. A femtosecond laser creates an intrastromal lenticule of precise shape and thickness according to the patient’s refractive error, which is then extracted through a very small incision, effectively flattening the patient’s cornea to correct myopia. Myopia from -1.00D to -10.00D can be treated, with additional cylindrical correction. The newly released Zeiss Visumax 800 also offers hyperopic treatment, as well as cyclotorsion assistance to optimise the treatment of astigmatism.
Early SMILE treatments suffered from slightly delayed visual recovery compared to LASIK, but constant optimisation of energy levels and spot spacing has significantly accelerated visual recovery. Visual outcomes, safety and quality-of-life data for the treatment of myopia are now comparable to LASIK2. This minimally invasive technique offers the advantage of maximum retention of anterior corneal innervation, hence it has faster recovery of corneal sensation and milder and shorter-lived dry eye symptoms compared to LASIK3. Furthermore, because SMILE preserves more of the anterior stroma, it results in superior structural integrity compared to LASIK4 and better spherical aberration control than LASIK5. Complications after SMILE are uncommon and very similar to LASIK, but without the lifelong risk of flap dislocation.
ICLs
The Staar Visian Implantable Collamer Lens, or Implantable Contact Lens (ICL), is an additive technology for correcting refractive error from -20D to +20D, including astigmatism, involving the insertion of a lens into the sulcus of a phakic patient whose corneas are too thin or irregular for laser surgery. Recognised post-operative complications such as cataract formation, pupil-block glaucoma and pigment dispersion glaucoma have significantly reduced with newer versions of the ICL. In a study of patients receiving the current EVO and EVO toric ICLs, 76% achieved unaided visual acuity of 6/6, with 99% achieving 6/9 or better after six months6.
Patients 40-60 years old
This is the most complex and challenging group to manage. Patients are either nearly presbyopic – with the disadvantage of not yet understanding the frustration of presbyopia, and hence the implications of wanting bilateral emmetropia – or are already presbyopic but often unrealistic about what can be achieved in terms of a range of perfect vision. Unlike the under 40s, who are largely myopes, this group has a significant number of emmetropes and hyperopes frustrated with the loss of near vision. These patients need very careful assessment to establish their aims, occupational visual requirements, hobbies and pastimes. The planning processes involved are multidisciplinary, with the patient’s optometrist often crucial in planning refractive targets. Patients often need to do contact lens trials of monovision, as well as possible trials of multifocal contact lenses, to get a basic idea about the potential visual side effects of multifocal IOLs.
Corneal laser
The same corneal laser surgical techniques are still applicable as for younger patients (PRK, LASIK, SMILE), but the complexity is the refractive target. Monovision is well tolerated by most patients7 and can be achieved by PRK, LASIK and SMILE, although steepening a cornea in a hyperopic eye tends to offer poorer visual quality than patients who are previously myopic. A significant number of patients may not adapt to contact lens monovision, or may desire excellent depth perception, limiting their laser-based options.
The precision of current excimer laser offers the opportunity of creating ‘multifocal corneas’, creating a central island in the cornea to provide near vision. However, there can often be a loss of distance vision. A better alternative is to manipulate the spherical aberration of the eye to increase the depth of focus, usually used to create a more tolerable monovision – an example of this is Presbyond (Zeiss)8.
Refractive lens exchange
The term ‘dysfunctional lens syndrome’ was coined to encompass presbyopia as well as the decreased contrast acuity and light scatter that occurs in the middle-aged group, without the lens being frankly cataractous9. Refractive lens exchange (RLE) in this age group may be the best way to improve both distance and near vision – a treatment which has been shown to be effective and safe with an incidence of serious adverse events less than 1%10.
There has been a significant advancement in the technology of multifocal IOLs, including bifocal and trifocal options, as well as extended depth of focus IOLs (EDOF IOLs). While a detailed description of available lenses is beyond the scope of this article, there are many IOL options, each with specific benefits and disadvantages in terms of range of vision, and possible visual side effects. The age at which RLE becomes the best option depends on both the patient’s desire for a ‘permanent’ solution to their presbyopia, as well as their existing refractive status.
For myopes, laser monovision is well tolerated and usually the treatment of choice until early/mid-50s, particularly as it may be wise to avoid RLE in high myopes until they have visually significant lens opacities due to the increased risk of post-operative retinal detachment. Hyperopes, on the other hand, start to lose distance vision as well as near vision with presbyopia, and correction of higher levels of hyperopia with laser tends to be less predictable, so RLE may be a good option even before 50 years old.
Patients require an extensive pre-operative work up, including a full assessment of their visual requirements and expectations, and accurate biometry and topography. The success of most multifocal and EDOF IOLs is dependent on hitting the refractive targets accurately, so it is mandatory the patient’s cornea is suitable for excimer laser enhancement post-operatively.
Patients over 60 years old
These patients were once a relatively easy group, but expectations of spectacle freedom are now high. Cornea-based refractive surgery alone is not usually an option, given that all patients in this group have cataract/lens opacities. They furthermore often have ocular comorbidities such as macular degeneration or glaucoma, which may reduce the potential best-corrected vision in one or both eyes, reducing the chance of success with monovision.
Multifocal/EDOF IOLs require regular corneas and healthy retinas to work, and even dry eye can reduce their effectiveness, so these lenses are often not appropriate. Assessment of the potential best option for patients is more limited, in that contact lens trials of monovision and multifocal lenses fail due to reduced best-corrected vision from the existing cataracts, although many patients may arrive having already done CLs monovision or successfully worn multifocal CLs for years. Again, in-depth counselling about options and realistic outcomes is mandatory and, just like in the middle-aged group, those receiving multifocal/EDOF IOLs ideally need to be assessed for suitability for any post-operative corneal laser surgery enhancements that may be required to achieve the best outcome. Alternatively, piggyback sulcus IOLs can be used to fine tune the refractive outcome.
References

Dr Sue Ormonde is a senior lecturer in the Department of Ophthalmology, University of Auckland, and a consultant ophthalmologist specialising in refractive, cataract and corneal surgery at Greenlane Clinical Centre and in private practice at Auckland Eye.