Caffeine is a popular psychostimulant that acts as an adenosine receptor antagonist at physiological concentrations. It is the most widely used drug in history, consumed daily by more than 70% of New Zealanders in the form of coffee, tea, chocolate and caffeinated soft drinks. It has been estimated that adults aged between 20 and 64 years are exposed to an average of 3.5mg of caffeine/kg body weight/day¹.
Historical studies suggest some ophthalmologists have long expressed concerns about the effect of caffeine on intraocular pressure (IOP) in glaucoma patients²,³. To date, IOP remains the only treatable risk factor in primary open angle glaucoma (POAG), the most common type of glaucoma. Thus, establishing the link between caffeine and IOP is of great importance for improving the management of POAG.
Effect of caffeine on IOP
A number of clinical trials have investigated the immediate effect of caffeine on IOP. The effect of caffeine has been regarded as controversial due to inconsistencies amongst study findings. These inconsistencies can be attributed to variable study protocols, such as sources and doses of caffeine, methods of tonometry and time points of IOP measurement. Additionally, participant characteristics and severity of glaucoma were often not clearly documented in some studies. Nonetheless, a careful review of the literature reveals a common trend.
In young and healthy volunteers without history of ocular diseases, no significant changes in IOP were detected up to four hours following ingestion of caffeine capsules⁴,⁵. One study, however, demonstrated a post-caffeine increase in IOP of 2-3 mmHg in healthy volunteers aged between 20 and 29 and this increase was maintained for three hours⁶. However, the volunteers drank a litre of coffee in this study and the authors did not delineate the effects of volume overload and high dose caffeine.
Several randomised controlled trials and subsequent meta-analysis of those studies reported IOP changes in patients with POAG or ocular hypertension following caffeine ingestion. There was a statistically significant increase in IOP when the patients were exposed to 180mg of caffeine in coffee, equivalent to approximately one double-shot espresso⁷-⁹ (see Table 1). The meta-analysis showed the weighted mean IOP differences before and after coffee consumption in patients with glaucoma or ocular hypertension: 0.347 at 30 minutes, 2.395 at 60 minutes and 1.998 at 90 minutes (95% confidence interval 0.078-0.616, 1.741-3.049, 1.522-2.474, respectively)⁷.
A major shortcoming of this meta-analysis is the lack of age-matched controls, leaving the effect of aging unknown. The healthy controls were mostly in their 20s. The age range of glaucoma patients were not stated in the papers but were expected to be in a much older age group. Furthermore, the authors did not differentiate high tension POAG from ocular hypertension, or normo-tension POAG, when they could represent distinct disease entities. Despite these weaknesses, the consensus is that caffeine, at least transiently, induces a small increase in IOP in glaucomatous eyes, but not in young healthy eyes.
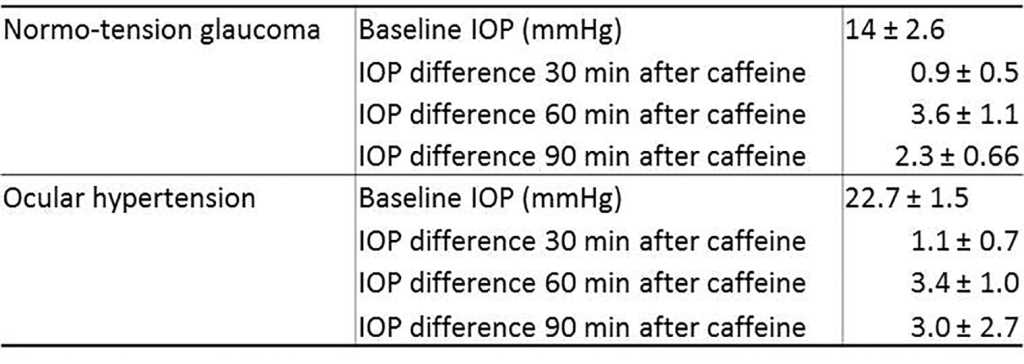
Table 1. Average IOP before and after caffeine ingestion in patients with normo-tension glaucoma and ocular hypertension
What is the pathophysiological significance of the IOP change?
Two large-scale epidemiologic studies addressed the question whether caffeine consumption is associated with the development or progression of glaucoma. The Blue Mountains Eye Study, a cross-sectional study conducted in Australia, investigated correlation between IOP and regular daily caffeine intake in POAG patients¹⁰. The participants completed questionnaires on their pattern of coffee consumption and underwent comprehensive glaucoma assessment. The study demonstrated a positive association between daily coffee drinking and high IOP, only in people with POAG. POAG patients who drank coffee daily had higher mean IOP (19.6mmHg) than those who did not (16.8mmHg). This result reached statistical significance after adjusting for age, sex, systolic blood pressure, myopia, current smoking and diabetes.
A large-scale prospective study of health professionals in the USA showed an association between coffee consumption and development of POAG in people with a family history of glaucoma¹¹. A large number of health professionals over 40 years of age and without a history of POAG were followed up for 18 years in this study. Daily caffeine intake of up to 600mg per day (approximately four double-shot espresso coffees or five cups of brewed coffee) was not associated with increased risk of developing POAG as shown by relative risks of around 1. With over 600mg of daily caffeine intake, the relative risk increased slightly to 1.61. Notably, in people with a family history of glaucoma, high caffeine intake of more than 600mg per day increased the relative risk from 0.94 to 2.01. In other words, people with a family history were twice as likely to develop POAG as those without, if they were heavy coffee drinkers (>600mg per day).
Taken together, there is still insufficient evidence to support caffeine as an independent risk factor for the development of POAG, but people with POAG or with a family history of glaucoma (ie. genetic susceptibility) may be more vulnerable to the effects of caffeine.
Mechanism of caffeine-induced IOP elevation
The main mechanism of caffeine’s effect is via adenosine receptor antagonism and subsequent increase in sympathetic tone and a slight elevation of blood pressure¹². In young and healthy volunteers, 200mg of oral caffeine led to significant retinal vasoconstriction one hour post-ingestion⁴This was negatively correlated with mean arterial pressure, suggesting an auto-regulatory response to increased blood pressure. Another study demonstrated that ingestion of 300mg of caffeine caused an increase in the resistive index of retrobulbar arteries in young and healthy volunteers¹³. Hypothetically, the increase in systemic blood pressure will increase pressure within the ciliary arteries, which in turn will increase ultrafiltration and aqueous production, thereby elevating IOP. Increased arterial pressure can also increase venous pressure and reduce aqueous clearance, thereby contributing to elevated IOP. Caffeine-induced vasoconstriction was however not associated with high IOP in the young and healthy, suggesting the presence of an unknown homeostatic mechanism to maintain the IOP.
Consequently, more questions arise as to why caffeine elevates IOP in only glaucoma patients. Several researchers postulate there may be an inherent susceptibility to the effect of caffeine in glaucomatous eyes. There is mounting evidence that vascular and autonomic dysfunction is a key pathologic process in glaucoma (for a comprehensive review, see reference 14). Doppler ultrasound imaging studies demonstrated that POAG patients failed to auto-regulate central retinal artery blood flow during postural change. Gene expression studies identified impairment of nitric oxide-mediated smooth muscle cell relaxation and excessive plasma levels of endothelin, a potent vasoconstrictor, in response to physiological perturbations in POAG patients. Polymorphisms of nitric oxide synthase and caveolin, which lead to impaired vasodilation, have been associated with POAG. Genetic dysautonomic conditions such as familial dysautonomia and nail-patella syndrome are associated with subtypes of POAG. Moreover, examination of the nail bed capillary network revealed abnormal peripheral microvascular circulation in glaucoma patients. It is possible that caffeine produces a pathologic haemodynamic response and consequent IOP change in glaucoma patients with structurally and functionally impaired microvasculature.
The debate continues…
Based on the evidence accumulated to date, glaucoma patients may be advised to avoid caffeine intake for 90 minutes before IOP measurement, in order to obtain a more accurate IOP reading. However, there is no known clinical benefit of avoiding caffeine in the long-term management of POAG and without clear evidence we are more likely to cause unnecessary anxiety associated with caffeine consumption. A few crucial questions remain to be answered before clinicians can make evidence-based recommendations on caffeine consumption.
These questions need to be addressed in future studies to establish evidence-based recommendations. In the meantime, it would be reasonable to advise patients to avoid excessive caffeine intake if IOP control is critical since even a small reduction in IOP has been shown to reduce the risk of glaucoma progression¹⁵.
References
1. Ministry for Primary Industries. Caffeine. New Zealand: 2012 November.
2. Leydhecker W. Influence of coffee upon ocular tension in normal and in glaucomatous eyes. Am J Ophthalmol. 1955 May;39(5):700-5.
3. Davis RH. Does caffeine ingestion affect intraocular pressure?. Ophthalmology. 1989 Nov;96(11):1680-1.
4. Terai N, Spoerl E, Pillunat LE, Stodtmeister R. The effect of caffeine on retinal vessel diameter in young healthy subjects. Acta Ophthalmol (Oxf). 2012 Nov;90(7):524.
5. Adams BA, Brubaker RF. Caffeine has no clinically significant effect on aqueous humor flow in the normal human eye. Ophthalmology. 1990 Aug;97(8):1030-1.
6. Okimi PH, Sportsman S, Pickard MR, Fritsche MB. Effects of caffeinated coffee on intraocular pressure. Appl Nurs Res. 1991 May;4(2):72-6
7. Li M, Wang M, Guo W, Wang J, Sun X. The effect of caffeine on intraocular pressure: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2011 Mar;249(3):435-42.
8. Higginbotham EJ, Kilimanjaro HA, Wilensky JT, Batenhorst RL, Hermann D. The effect of caffeine on intraocular pressure in glaucoma patients. Ophthalmology. 1989 May;96(5):624-6.
9. Avisar R, Avisar E, Weinberger D. Effect of coffee consumption on intraocular pressure. Ann Pharmacother. 2002 Jun;36(6):992-5.
10. Chandrasekaran S, Rochtchina E, Mitchell P. Effects of caffeine on intraocular pressure: the Blue Mountains Eye Study. J Glaucoma. 2005 Dec;14(6):504-7.
11. Kang JH, Willett WC, Rosner BA, Hankinson SE, Pasquale LR. Caffeine consumption and the risk of primary open-angle glaucoma: a prospective cohort study. Invest Ophthalmol Vis Sci. 2008 May;49(5):1924-31.
12. James JE. Critical review of dietary caffeine and blood pressure: a relationship that should be taken more seriously. Psychosom Med. 2004;66(1):63-71.
13. Ozkan B, Yuksel N, Anik Y, Altintas O, Demirci A, Caglar Y. The effect of caffeine on retrobulbar hemodynamics. Curr Eye Res. 2008 Sep;33(9):804-9.
14. Pasquale LR. Vascular and autonomic dysregulation in primary open-angle glaucoma. Curr Opin Ophthalmol. 2016 Mar;27(2):94-101.
15. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E, et al. Factors for glaucoma progression and the effect of treatment: the early manifest glaucoma trial. Arch Ophthalmol. 2003 Jan;121(1):48-56.
Dr Jinny Yoon is a neuro-ophthalmology research fellow. She studied neuroscience at the University of Auckland and graduated with a PhD. After completing basic medical training in Auckland, she followed her passion for eye health and joined the Department of Ophthalmology.
Professor Helen Danesh-Meyer is an international authority on glaucoma and neuro-ophthalmology, chair of Glaucoma NZ and the Save Sight Society, is a sought after international speaker, has published more than 120 articles and is a respected international journal editor.