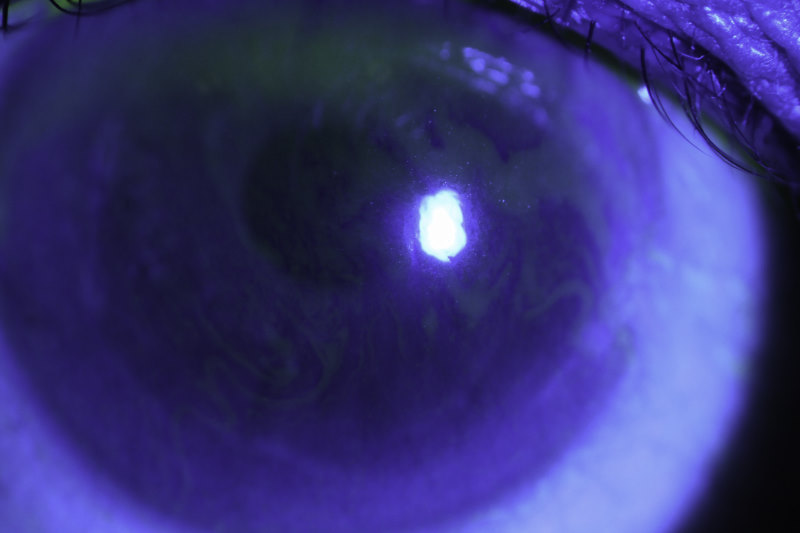
Deficiency in tear film quality and quantity are often considered key defining characteristics of dry eye disease (DED). The complex, dynamic multi-component structure, which comprises an underlying aqueous-mucous layer and a superficial lipid layer, synergistically maintains ocular surface homeostasis. Functionally, the aqueous-mucus layer is believed to improve the wettability and support corneal adhesion of the tear film, while the lipid layer tends to form a superficial protective “blanket”, providing an occlusive effect. “Holes” in the blanket (see Fig 1), as typically observed in evaporative DED and especially in meibomian gland dysfunction, can increase exposure of the underlying aqueous layer of the tear fluid to the environment and evaporation, leading to hyperosmolarity of the tear film and epithelial apoptosis. Consequently, artificial tears are frequently used for the management of tear film deficiencies. However, the term “artificial tears” is a misnomer as most products do not mimic the complex composition of human tears and contrary to their name, they typically “supplement” rather than “replace” the tear fluid.
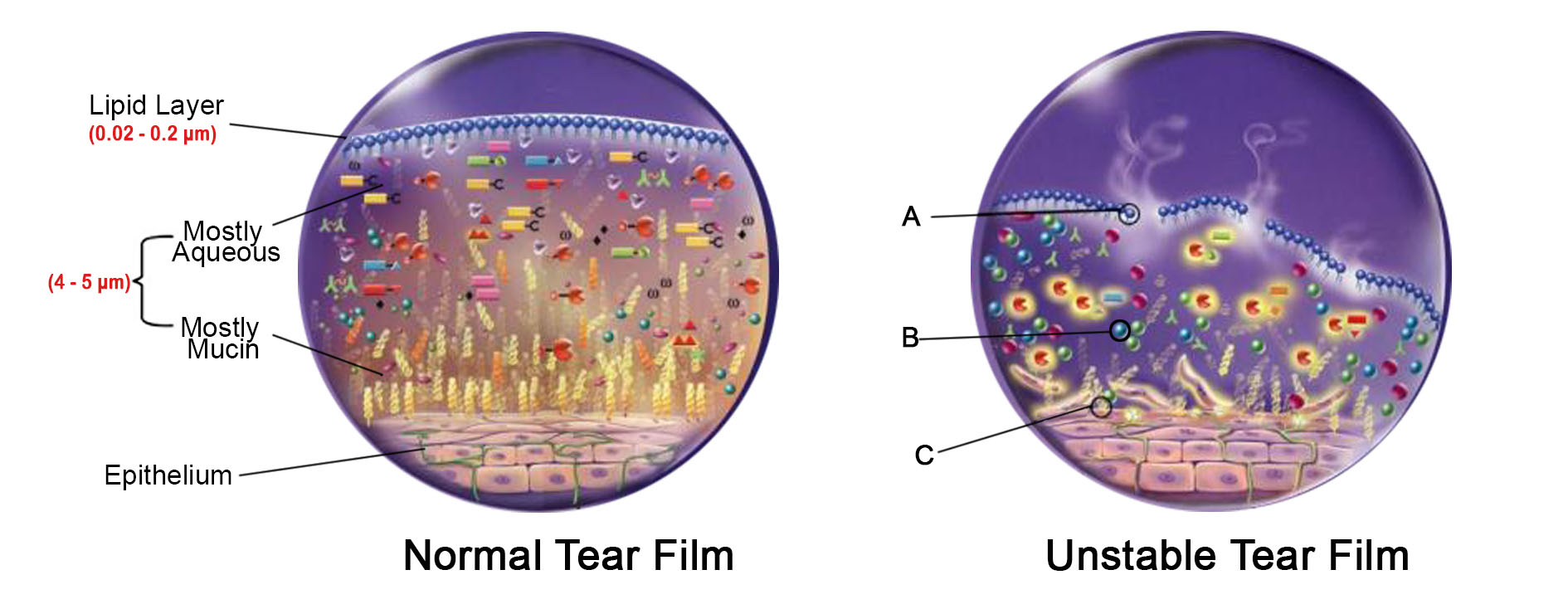
Fig 1. Healthy tear film (left) and unstable tear film (right), typically characterised by (A) a discontinuous lipid layer, (B) a hyperosmolar aqueous layer and (C) reduced mucins and goblet cells
Artificial tear supplements can be isotonic or hypotonic aqueous eye drops, which may have additional viscosity building agents such as carboxymethylcellulose (Refresh, Allergan), hydroxypropyl guar (Systane, Alcon) or sodium hyaluronate (Hylo-Forte, AFT Pharmaceuticals). They typically function by augmenting the aqueous layer and transiently reducing tear fluid osmolarity; however, their effect is generally short-lived due to rapid drainage and evaporation from the ocular surface. Osmoprotective agents, such as trehalose and erythritol (believed to reduce the concentration of intracellular organic salts without disturbing cellular macromolecular components) may also be added to aqueous eye drops to reduce hyperosmolar stress. On the other hand, lipid-based eye drops, which generally contain amphiphilic lipids and/or surfactants, fortify the tear film lipid layer to inhibit excessive evaporation.
Lipid-based artificial tear supplements are generally believed to have a more sustained effect than non-lipid eye drops and may be superior in the management of DED, especially when it is associated with meibomian gland dysfunction. For instance, instillation of lipid-based eye drops has shown a significantly greater improvement in tear film lipid layer thickness and consequent reduction in tear evaporation in patients with DED, resulting in superior prophylactic efficacy on exposure to desiccating environmental stress.
Consequently, several lipid-based artificial tear supplements have been developed with the objective of reducing tear evaporation and providing long-term relief to patients with dry eyes. Lipid-based eye drops are most frequently available in the form of oil-in-water emulsions such as Cationorm (Santen SAS) or ointments such as VitA-POS (AFT Pharmaceuticals). Liposomal sprays such as Optrex ActiMist (Optima Pharmazeutische), which potentially improve tear film integrity by replenishing the phospholipid layer at the aqueous-lipid interface, have also shown significant improvement in tear film quality.
A significant concern with long-term eye drop use, however, is the presence of irritating preservatives, which can compromise the ocular surface and worsen patient discomfort. Surfactants typically used to prepare oil-in-water lipid-based eye drops may also exacerbate dry eye symptoms by transiently destabilising the tear film. Consequently, several surfactants have been listed in the TFOS DEWS II iatrogenic report as agents that potentially cause dry eye. In an attempt to avoid such components, a preservative-free lipid layer stabilising eye drop has recently been developed by Novaliq using a novel, optically transparent, non-aqueous, semifluorinated alkane. This product is currently marketed as EvoTears (Ursapharm) in Europe and as NovaTears (AFT) in Australia and New Zealand and has shown promising results in multi-centre clinical trials performed in patients with evaporative dry eye disease. Recent research has also shown that semifluorinated alkanes can be used as a vehicle for delivery of therapeutic agents to the eye5 and potentially simplify the dosage regimen for patients with chronic dry eye disease.
References
1. Gokul A, Wang MTM, Craig JP. Tear lipid supplement prophylaxis against dry eye in adverse environments. Contact Lens and Anterior Eye. 2017.
2. Craig JP, Purslow C, Murphy PJ, et al. Effect of a liposomal spray on the pre-ocular tear film. Contact Lens and Anterior Eye. 2010;33(2):83-7.
3. Gomes JAP, Azar DT, Baudouin C, et al. TFOS DEWS II iatrogenic report. The Ocular Surface. 2017;15(3):511-38.
4. Steven P, Scherer D, Krösser S, et al. Semifluorinated Alkane Eye Drops for Treatment of Dry Eye Disease--A Prospective, Multicenter Noninterventional Study. Journal of Ocular Pharmacology and Therapeutics. 2015;31(8):498-503.
5. Agarwal P, Scherer D, Günther B, et al. Semifluorinated alkane based systems for enhanced corneal penetration of poorly soluble drugs. International Journal of Pharmaceutics. 2018;538(1):119-29.
Dr Priyanka Agarwal is currently a research fellow in the University of Auckland’s School of Pharmacy. Her research interests include drug delivery and bench-to-bedside formulation development. Dr Ilva Rupenthal is a senior lecturer in the University of Auckland’s Department of Ophthalmology and director of the Buchanan Ocular Therapeutics Unit (www.botu.nz), which aims to translate ocular therapeutic-related scientific research into the clinical setting. Disclosure: Dr Agarwal’s doctoral studies, supervised by Dr Rupenthal, were funded by Novaliq GmbH, manufacturer of NovaTears.