


The Canterbury Low Vision Clinic at Burwood Hospital, Christchurch, is a centre of excellence for the rehabilitation of people with various debilitating eye conditions and, over the years, it has received regular referrals of patients with homonymous hemianopia (HH).
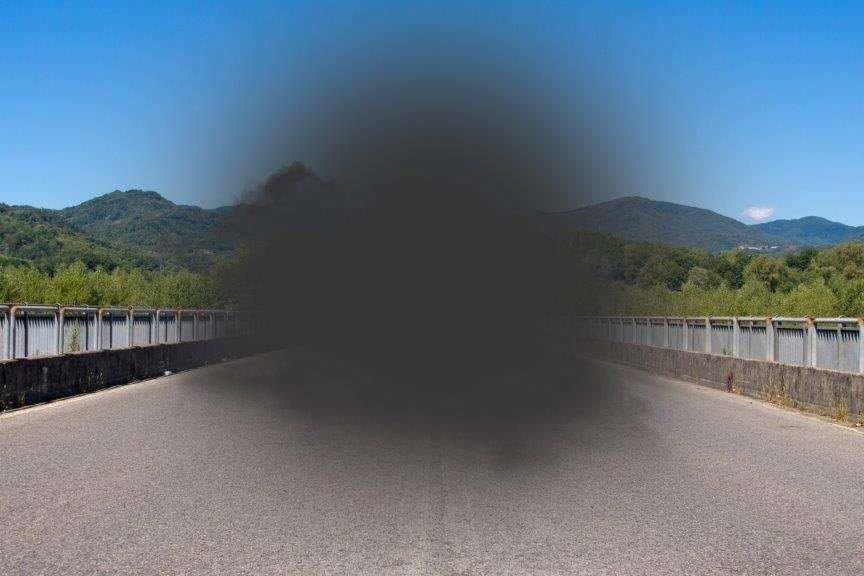
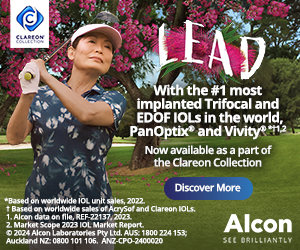
HH is a condition involving vision loss on the same side of the visual field in both eyes. The effect stems from a problem in brain function, not vision, and is indicative of a lesion involving the visual pathway posterior to the chiasm. Although often caused by stroke, HH can arise from any disorder affecting the brain, including tumours, inflammation and injuries.
While diagnosing HH in a visual field exam is straightforward, it is very difficult for the patient and whānau to understand the disorder’s causes and consequences, and viewing a Humphrey field test can be confusing to patients. There is often a sense of denial, which has to be overcome to successfully manage HH.
To help the patient and whānau understand the extent of the vision loss, it can be useful to perform the Hamilton-Veale Laser Field Test in clinic. Allowing the patient’s accompanying person to plot the vision loss is a helpful way for everyone to understand what’s going on. As practitioners, we should explain to the patient that the majority of cases do not recover, so learning compensatory techniques is essential, as is understanding why the stroke has caused the field loss. To explain why it has affected both eyes, we can offer patients a colour-coded visual pathway and point out the loss is not in the eyes but in the brain.
Treatment by a low-vision specialist deals with two main areas: navigating the environment and improving reading ability. Helpful techniques for patients and the people they spend time with include:
Christchurch-based optometrist John Veale is a low-vision patient advocate and a long-serving member of NZ Aid’s (New Zealand Agency for International Development) eye team.