



The prevalence of keratoconus in Aotearoa New Zealand is purported to be higher than the global average1. This has been attributed to Aotearoa having the largest number of Māori and Pasifika worldwide2; populations within which the prevalence of keratoconus has been suspected to be disproportionately high (Fig 1)2-4. Government census figures recorded the number of Pasifika in Aotearoa in 2018 at 381,642, encompassing more than 40 distinct ethnic groups5. Pasifika are projected to undergo significant population growth over the next two decades, bringing with it a potential rise in keratoconus cases.
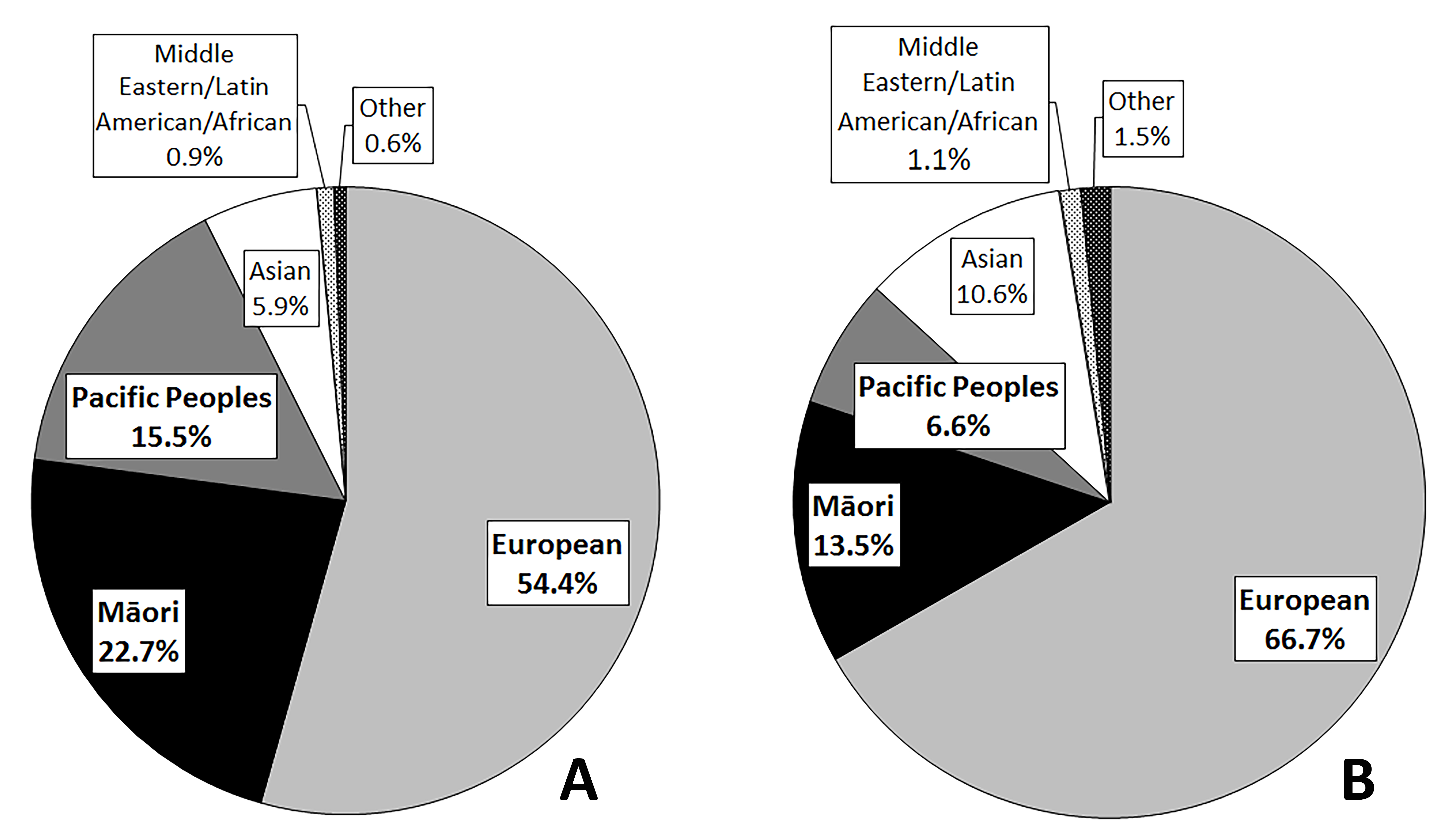
Fig 1. Ethnic distribution. Left, all cases of Keratoconus in the ARK study (N=1,869). Right, all individuals captured in the 2013 New Zealand Census2
Keratoconus carries particular significance in that disease onset generally occurs in late childhood or early adolescence, impacting visual acuity, quality of life and potentially the ability to obtain an education and maintain employment. Severe disease can result in negative effects across a wide metric of other health and wellbeing measures, further exacerbating inequities.
The data available on keratoconus and Pasifika
Pasifika health inequities in Aotearoa have been recorded extensively across a wide range of health issues6. The available figures on keratoconus, however, remain profoundly scant in comparison. A brief scope of the literature found only a handful of articles covering the subject. Indeed, the incidence of keratoconus across all population groups in Aotearoa has yet to be accurately quantified. The articles identified on the topic were all published in Aotearoa, with none identified from neighbouring Oceanic states.
These studies all lent weight to the observation that Pasifika are disproportionately impacted by keratoconus. The majority of these note an overrepresentation of Pasifika in their sample populations relative to the proportion of Pasifika in the general population7-9. Māori/Polynesians, were found to be twice as likely to exhibit suspect or anomalous corneal topography, compared to non-Māori/Polynesian students in one study3. Studies reviewing keratoconus severity found Māori or Pacific ethnicity to be associated with more severe keratoconus and a younger mean age at diagnosis10. The Aotearoa Research into Keratoconus (ARK) study supports these observations, noting Māori and Pasifika as having the highest proportion of eyes graded in most severe category, as well as the lowest proportion of patients in the least severe category of keratoconus9.
Pasifika in Aotearoa are also disproportionately impacted by keratoconus complications. The Auckland keratoconus study noted Pacific ethnicity, as an independent risk factor for developing acute corneal hydrops (Fig 2). In the same study, 43% of corneal transplants for keratoconus performed were on Pasifika patients, despite Pasifika representing only 7% of the New Zealand population11. A 10-year review of corneal transplantation cases in Auckland (1999-2009) also noted within their keratoconic group sample there was a significantly higher proportion of Pasifika relative to the general population12.
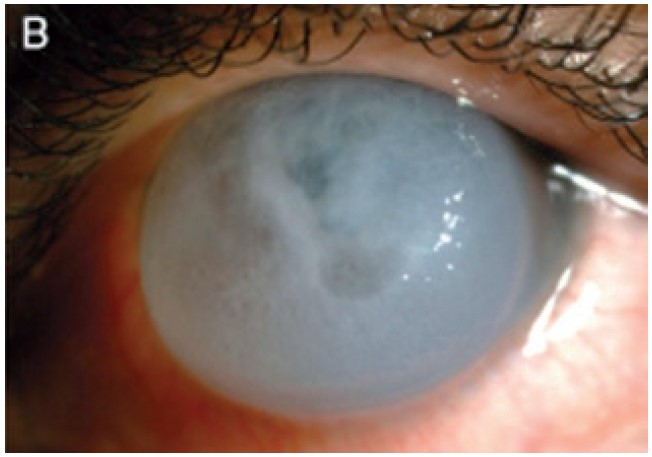
Fig 2 B. Severe acute corneal hydrops in keratoconus in a 16-year-old subject who had initially presented with keratoconus only six months earlier
Familial history of disease was also found to be more common in Pasifika, Māori and Asian patients than in Europeans4. Some, however, note the contrary but attribute this to a lack of disease awareness among Pasifika population groups and lower health literacy rates3.
Why the disproportionate rates of disease?
Documented risk factors for keratoconus include a history of atopy (hayfever, asthma, eczema), eye rubbing or family history. Rates of atopy in Aotearoa are noted to be among the highest in the world13. Māori and Pasifika, however, are more disproportionately impacted, with both groups recorded to have the highest rates of children with medicated asthma of any ethnic group in the country14. Established socioeconomic determinants of health are major influences of these risk factors, with Pasifika concomitantly being impacted by a relative overrepresentation in the lower socioeconomic deciles15, higher rates of overcrowded housing, poor health literacy6 and reduced accessibility of existing ocular health and health screening services16. Students in low-decile schools, for instance, were found to be more likely to develop keratoconus than students in higher decile schools17. Lapses in follow-up attendance after treatment potentiate these disparities further, with Māori and Pasifika patients found to have the lowest rates of follow-up attendance after penetrating corneal transplants, independent of their level of social deprivation7. A recent prospective study among keratoconus patients in Auckland also noted Māori and Pasifika patients to have the highest rates of non-attendance to the Auckland Crosslinking Service, despite presenting younger and with greater disease severity and poorer visual acuity18.
The work to be done
As a result of these disparities, targeted screening measures have been proposed for teenagers of Māori and Pasifika descent2, although only a small fraction of these appear to have been implemented. Interventions aimed at achieving equity of eye health outcomes among Pasifika will require direct leadership and guidance from within our Pasifika communities, with subsequent provision of services that align with established Pasifika models and methodologies.
Existing health strategies have often failed to employ pivotal, intricately interconnected Pasifika community networks in the planning and delivery of proposed interventions. Pasifika community engagement, for instance, hinges on cultural and faith-based settings. Churches remain a significant focal point for Pasifika, with pastors (faife’au, faifekau or talatala) also taking on the roles of cultural and community leaders. Their influence has significant potential in promoting health and health awareness for their congregations.
Traditional hierarchies, through the family or village units, are also crucial in ensuring adequate service delivery or dissemination of knowledge throughout our Pasifika communities. Informing chiefs, community leaders and elders through fono (meetings or cultural gatherings, particularly in church settings) can have a massive role in bolstering community engagement to ensure these disparities are addressed more effectively.
Effective service delivery and health promotion for Pasifika ultimately ensures they hear from people they trust – people who embody the cultural values consistent with their worldviews. In the Tongan context, which my heritage affords me the ability to articulate, these revolve around deeply rooted systems of faka’apa’apa (respect), lototo (humility), mamahi’i me’a (passion for community and country) and tauhi vaha’a (reciprocity) among a plethora of others.
In a video discussing the recent major health system reforms and Pasifika communities, the former minister of Pacific peoples, Aupito Sua William Sio, reiterated the need for people in the health sector who “speak our language”. He also said the health system needs “our cultural values and perspectives reflected in models of care and service delivery”, employing modes of participatory health research or co-design that work with our people rather than ‘on’ them19.
Interventions aimed at correcting health inequity for Pasifika, including keratoconus, will need to ensure these understandings are embodied and valued, reflecting the values that foster trust and in turn, improve outcomes. Regional knowledge-sharing will be crucial in allowing translation of these benefits across the wider Oceanic region as well, ultimately ensuring that, Tākanga ‘etau fohe (‘Our oars paddle in unison’) – a Tongan proverb.
References
1. Patel D, McGhee C. Understanding keratoconus: what have we learned from the New Zealand perspective? Clin Exp Optom 2013;96(2):183-187.
2. Gokul A. Characterising and modifying the keratoconus disease process in New Zealand – The Aotearoa research into keratoconus (ARK) ProjectResearchSpace@ Auckland; 2017.
3. Owens H, Gamble G, Bjornholdt M, Boyce N, Keung L. Topographic indications of emerging keratoconus in teenage New Zealanders. Cornea 2007;26(3).
4. Jordan C, Zamri A, Wheeldon C, Patel D, Johnson R, McGhee C. Computerized corneal tomography and associated features in a large New Zealand keratoconic population. Journal of Cataract & Refractive Surgery 2011;37(8):1493-1501.
5. Stats NZ. Pacific Peoples Ethnic Group. 2018; Available at: https://www.stats.govt.nz/tools/2018-census-ethnic-group-summaries/pacific-peoples.
6. Tofa Saili: A review of evidence about health equity for Pacific Peoples in New Zealand. 2019 -07.
7. Crawford A, Krishnan T, Ormonde S, McGhee C, Patel D. Treatment adherence after penetrating corneal transplant in a New Zealand population from 2000 to 2009. Cornea 2015;34(1):18-22.
8. Fan Gaskin J, Good W, Jordan C, Patel D, McGhee C. The Auckland keratoconus study: identifying predictors of acute corneal hydrops in keratoconus. Clinical and Experimental Optometry 2013;96(2):208-213.
9. Gokul A, Ziaei M, Mathan J, Han J, Misra S, Patel D, et al. The Aotearoa research into keratoconus study: geographic distribution, demographics, and clinical characteristics of keratoconus in New Zealand. Cornea 2022;41(1):16-22.
10. Niederer R, Perumal D, Sherwin T, McGhee C. Laser scanning in vivo confocal microscopy reveals reduced innervation and reduction in cell density in all layers of the keratoconic cornea. Investigative ophthalmology & visual science 2008 Jul 01,;49(7):2964-2970.
11. Fan Gaskin J, Good W, Jordan C, Patel D, McGhee C. The Auckland keratoconus study: identifying predictors of acute corneal hydrops in keratoconus. Clinical and Experimental Optometry 2013;96(2):208-213.
12. Crawford A, McKelvie J, Craig J, McGhee C, Patel D. Corneal transplantation in Auckland, New Zealand, 1999-2009: indications, patient characteristics, ethnicity, social deprivation, and access to services. Cornea 2017;36(5):546-552.
13. Asher M, Barry D, Clayton T, Crane J, D'Souza W, Ellwood P, et al. The burden of symptoms of asthma, allergic rhinoconjunctivitis and atopic eczema in children and adolescents in six New Zealand centres: ISAAC Phase One. N Z Med J 2001;114(1128):114-120.
14. Ministry of Health NZ. Annual Data Explorer 2020/21: New Zealand Health Survey 2022. Available at: https://minhealthnz.shinyapps.io/nz-health-survey-2021-22-annual-data-explorer/.
15. Boven N, Exeter D, Sporle A, Shackleton N. The implications of different ethnicity categorisation methods for understanding outcomes and developing policy in New Zealand. Kōtuitui 2020 Jan 02,;15(1):123-139.
16. Jaymie Tingkham Rogers, Joanna Black, Matire Harwood, Ben Wilkinson, Iris Gordon, Jacqueline Ramke. Vision impairment and differential access to eye health services in Aotearoa New Zealand: protocol for a scoping review. BMJ Open 2021;11(9):e048215.
17. Papali'i-Curtin AT, Cox R, Ma T, Woods L, Covello A, Hall RC. Keratoconus prevalence among high school students in New Zealand. Cornea 2019;38(11):1382-1389.
18. Angelo L, Gokul A, Wadhwa H, McGhee CNJ, Ziaei M. Assessment of barriers to accessing a first specialist assessment and follow-up keratoconus and crosslinking service at a tertiary referral centre to address health disparities. Cornea 2023;Publish Ahead of Print.
19. Labour Pāsifika Caucus. Health NZ Reform, Minister Sio. 2022; Available at: https://fb.watch/h811Lyu4cE/.

Dr Hāʻano Fonua is a PGY2 house officer working at Middlemore Hospital with Te Whatu Ora Counties Manukau in Auckland. He is of Tongan descent from the villages of ‘Utulau, Vainī, Fo’ui, Kolonga, Fakakakai and Hāʻano. His research interests include keratoconus, Pasifika ocular health and Pasifika health equity.

Dr Akilesh Gokul is a therapeutically qualified optometrist and a senior lecturer in Auckland University’s ophthalmology department. A clinician-scientist working with Te Whatu Ora’s public crosslinking service, his main research interests include keratoconus, contact lenses, crosslinking and inequity in healthcare.