









The most exciting developments in uveitis are advances in imaging techniques which can complement the clinical examination and assist in the formulation of a treatment strategy for patients with inflammatory eye diseases.
Quantitative analysis of vitreous inflammation using OCT in patients receiving sub-Tenon's triamcinolone acetonide for uveitic cystoid macular oedema, Sreekantam et al.
Br J Ophthalmol. 2017 Feb;101(2):175-179
Review:
This was a retrospective longitudinal study of 22 eyes. The investigators collected OCT images with the Heidelberg Spectralis in patients with uveitic cystoid macular oedema before and after treatment with sub-Tenons triamcinolone. Custom-built software was used to quantify vitreous opacification by measuring the vitreous signal intensity relative to the RPE signal intensity. This theoretically minimises the confounding factors of anterior media opacities as the vitreous signal is being directly compared to the RPE signal on the same scan.
OCT scans were obtained between four to 19 weeks after treatment, with a median time of seven weeks. The results showed a significant reduction in the VIT/RPE relative intensity after treatment. VIT/RPE relative intensity was also associated with a significant reduction in the mean central retinal thickness with a correlation coefficient of 0.53 (p=0.01), and a significant improvement in visual acuity, with a correlation coefficient of 0.702 (p=0.0001).
Comment:
Though this was a small observational study without a control group, it demonstrated that a novel objective parameter can be used to quantify vitreous inflammation, which is difficult to do clinically, and is graded qualitatively by the standardisation of uveitis nomenclature (SUN) working group based on clarity of fundal features. Despite the fact that clinical decision making about treatment is still based on retinal thickness and visual acuity, VIT/RRPE relative intensity can potentially be used as an adjunct to grade response, monitor the course of inflammation and compare effectiveness of different treatment methods in a single patient. What this study does not assess is repeatability, sensitivity and specificity and a larger cohort of patients against a control group.

Fig 1. Quantitive assessment of vitreous inflammation using optical coherence tomography (OCT) demonstrated in a
47-year-old male with intermediate uveitis (A and B) and a 48-year-old female with panuveitis (C and D)
Comparing OCT findings in different aetiologies of infectious necrotising retinitis, Invernizzi et al.
Br J Ophthalmol. 2018 Apr;102(4):433-437
Review:
This is a retrospective observational study where 23 eyes with infectious necrotising retinitis underwent OCT scanning with the Heidelberg HRA Spectralis. Features were compared according to aetiology. The cases were divided into a viral retinitis group, including VZV and CMV retinitis (13 eyes), and a toxoplasmosis group (10 eyes). The cases were diagnosed clinically, if there was ambiguity in the clinical findings a vitreous tap was performed and the sample underwent PCR testing for confirmation.
The common features on OCT of all the eyes examined were full thickness retinitis indicated by full thickness signal hyper-intensity and obscuration of the retinal layers, some degree of vitritis and thickening of the choroid underneath the lesion. The differentiating features found in patients with toxoplasmosis include: large hyper-reflective oval deposits on the retinal surface, retro-hyaloid space and posterior hyaloid surface. In the toxoplasmosis cases, the underlying choroid showed significant hypo-reflectivity with increased thickening and disruption of the architecture indicated by loss of septae on extended depth imaging scans. The differentiating features found in patients with viral retinitis were cystic oedema and hyper-reflective vertical stripes in the outer nuclear layer. Though these findings were significantly associated with viral aetiologies, they were relatively infrequent, present in only 38% of eyes in the viral group. These findings may be explained by the pathophysiology of toxoplasmosis chorioretinitis, in that it is highly inflammatory hence the presence of these ovoid deposits in the posterior segment, and that there is a greater involvement of the choroid compared to viral retinitis where there is mild choroidal thickening only.
Comment:
Once again, this is an observational uncontrolled study in a small number of eyes, however an interesting concept into some differentiating features which could help clinch the diagnosis early in some cases. It does not, however, absolve the need for aqueous humour or vitreous sampling and PCR testing for confirmation, and treatment with intra-vitreal anti-viral medication such as Foscarnet if acute fulminant viral retinal necrosis is suspected.
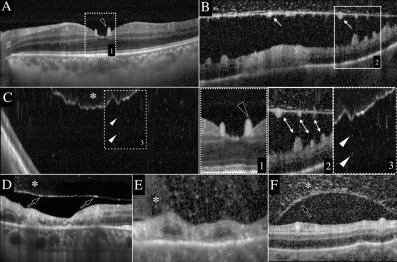
Fig 2. A, B and C are scans of patients with toxoplasmosis. E and F are scan of
patients with viral retinitis
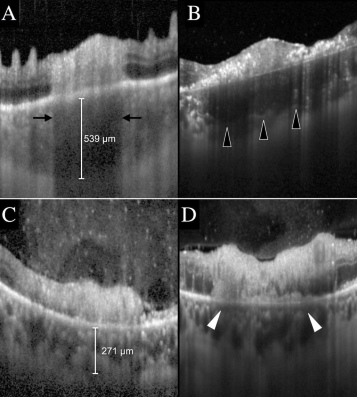
Fig 3. A and B are patients with toxoplasmosis, C and D are scans of patients
with viral retinitis
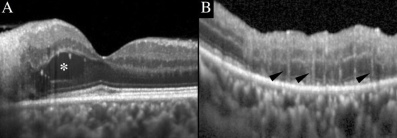
Fig 4. A and B are scans of patients with viral retinitis
Choroidal neovascularisation on OCTA in punctate inner choroidopathy and multifocal choroiditis, Levison et al.
Br J Ophthalmol. 2017 May;101(5):616-622
Review:
This was a prospective consecutive case series of 12 patients with multifocal choroiditis or punctate inner choroidopathy with known choroidal neovascularisation. All patients underwent a detailed slit lamp exam, spectral domain OCT imaging (Cirrus (V.6.1), Zeiss). Five patients underwent fluorescein angiography. All patients underwent OCT angiography (OCTA) with the Optovue Avanti-RTVue-XR.
OCTA identified a CNVM in 15 eyes of 11 patients, the appearance was of a hyper-reflective network of vessels at the choriocapillaris. In patients who underwent fluorescein angiography, a CNVM was identified in only four of seven eyes. In the other three eyes, there was abnormal staining but no clearly defined CNVM. OCTA demonstrated a clear CNVM in all these eyes with detail of the size and shape of the lesions.
OCTA was also able to demonstrate CNVM in patients where OCT scanning showed a PED with subretinal or sub-RPE hyper-reflective material, as well as patients with hyper-reflective subretinal material only and no PED. Indicators of CNVM activity were also identified as an increase in lesion size and less distinct vasculature.
Comment:
This was a small observational study which demonstrated findings that can form the basis for larger studies. OCTA may serve as a great tool to differentiate CNVM from inflammatory chorioretinal lesions due to an obfuscated appearance on OCT imaging alone, infrequent presence of intra-retinal or subretinal fluid and equivocal appearance on FA.
Larger controlled studies comprising of fundal photographs, OCT imaging, OCTA, FA and ICGA are needed to confirm these findings. Furthermore, OCTA does not provide information about vascular leakage and areas of non-perfusion in the peripheral retina, hence FA is here to stay in the investigative approach to posterior uveitis.
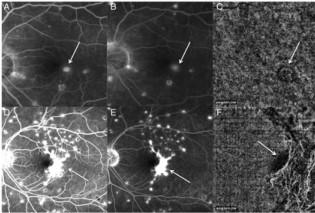
Fig. 5 Images of fluorescein angiography (FA) and corresponding optical coherence tomography
angiography (OCTA) are shown
Images courtesy of Br J Ophthalmology
About the author
Dr Noor Ali is an uveitis and glaucoma fellow at Auckland District Health Board.















