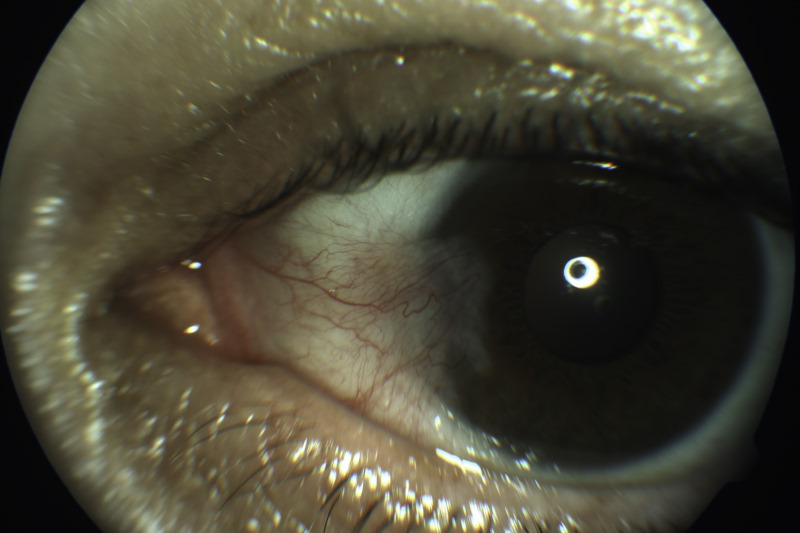
A pterygium is a common benign ocular surface growth. It typically starts on the nasal conjunctiva close to the limbus as a pinkish, triangular tissue growth and extends across the cornea. The cornea is susceptible to ultraviolet (UV) radiation due to its exposed position at the front of the eye, its shape and its natural transparency, which lead to a peripheral UV-focusing effect on the nasal limbus. There, the UV radiation is amplified by a factor of 20. Chronic UV light exposure is a known cause of degenerative deposition of subepithelial collagen fibres (scar), which eventually leads to pterygium development. Often both eyes are involved. Pterygia are progressive and slowly grow over time, but rarely so large that the pupil is covered.
Symptoms
Symptoms caused by pterygia vary widely from being barely detectable, to causing frequent redness, dryness, irritation and often blurred vision. The blurred vision is most frequently caused by distortion of the cornea and astigmatism, rather than occlusion of the visual access as the pterygium grows across the cornea. Severe sub-epithelial scarring may rarely cause ocular motility disturbance. Pterygia often result in significant cosmetic concerns.
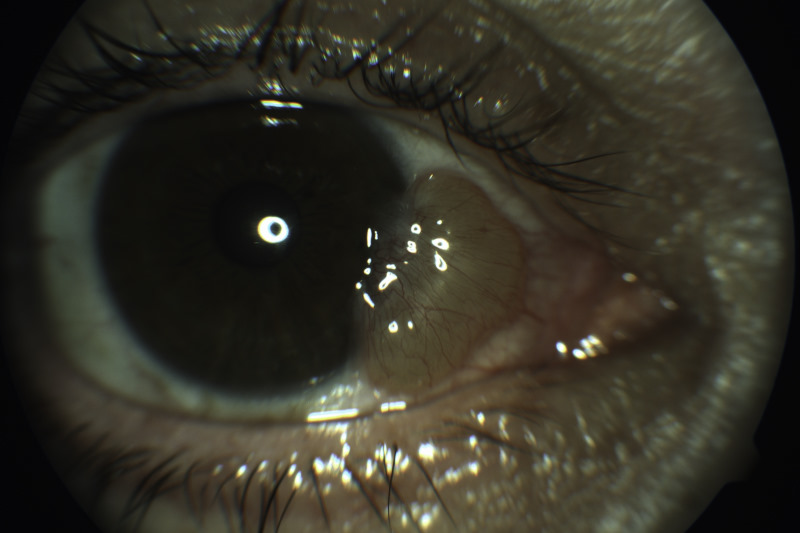
Elevated pterygium, likely to require surgical excision
Risks
The prevalence of pterygia varies from 1% to 53% in various regions of the world. The incidence is greater in locations close to the equator and at higher altitudes. China has the highest reported prevalence of pterygia. They occur more commonly among males than females, in those with an outdoor occupation, in smokers and those with higher alcohol consumption. The condition becomes more common with age and the incidence of pterygia appears to be more common in dark-skinned populations such as Pacific Island races rather than Europeans.
Risk reduction
You can help minimise symptoms and reduce the chances of a pterygium growing by reducing your UV light exposure: wear a wide-brimmed hat and sunglasses, all year round, and be especially careful during high-risk activities such as snow sports and water sports; avoid irritants which dry the eye, such as dusty and air-conditioned environments; use artificial tears regularly to lubricate the eye; reduce alcohol intake; and try and stop smoking.
Treatment
Among those with the condition, an eye lubricant can help with symptoms. Occasionally non-steroidal or steroid eye drops are prescribed for short-term management of inflammation. These are not recommended as a long-term treatment, however, due to serious side-effects.
With recurrent or severe irritation, if vision is threatened, and for those with unacceptable cosmesis, surgical treatment is recommended. Surgery involves removing the abnormal scar tissue and covering the bare sclera with a conjunctival graft. The graft is usually taken from the patient’s own conjunctiva from the sun-protected area under the top eyelid. This is usually performed under local anaesthetic as a day case. Post-operatively, patients require steroid eyedrops and careful follow-up.
Pterygia may recur, although surgery with conjunctival allografting reduces recurrences from approximately 30% to <5% and is now undertaken routinely in most cases. Commonly, the conjunctival graft is adhered to the bare scleral bed with fibrin glue made from blood donor products, rather than sutures, and the evidence suggests this further reduces recurrence rates. Occasionally, for recurrent or severe pterygia, ophthalmologists may apply the anti-metabolite mitomycin C intra-operatively.
Differentials
Ocular surface squamous neoplasia (OSSN) is a condition which can mimic pterygia. It is important to consider this in any patient presenting with a conjunctival mass extending to the limbus. Dysplastic lesions are often more vascularised and have a gelatinous, papillary or leukoplakic appearance compared to a pterygium. OSSN requires biopsy for confirmation of the diagnosis and grading of the severity.
References
Bradley JC, et al. The science of pterygia. Br J Ophthalmol. 2010;94:815–820.
Zhou WP, et al. The role of ultraviolet radiation in the pathogenesis of pterygia (Review) Mol Med Rep. 2016 Jul;14(1):3-15. Epub 2016 May 9.
Rezvan F, et al. Prevalence and risk factors of pterygium: a systematic review and meta-analysis. Surv Ophthalmol. 2018 Sep - Oct;63(5):719-735.
Sopoaga F, et al. Causes of excess hospitalisations among Pacific peoples in New Zealand: implications for primary care. J Prim Health Care. 2010;2:105–110.
Notara M, et al. UV light-blocking contact lenses protect against short-term UVB-induced limbal stem cell niche damage and inflammation.Sci Rep. 2018 Aug 22;8(1):12564.
Clearfield E, et al. Conjunctival autograft for pterygium.
Cochrane Database Syst Rev. 2016 Feb 11; 2:CD011349. Epub 2016 Feb 11.
Romano V, et al. Fibrin glue versus sutures for conjunctival autografting in primary pterygium surgery. Cochrane Database Syst Rev. 2016 Dec 2. Epub 2016 Dec 2.
Fonseca EC, et al. Comparison among adjuvant treatments for primary pterygium: a network meta-analysis. Br J Ophthalmol. 2018 Jun;102(6):748-756. Epub 2017 Nov 16.
Dr Rebecca Stack is an ophthalmologist and director at Southern Eye Specialists in Christchurch and the current director of ophthalmology at Christchurch DHB.