


Keratoconus is a non-inflammatory corneal degeneration that leads to progressive corneal thinning, myopia, irregular astigmatism and scarring, resulting in debilitating vision loss which affects patients' quality of life1,2. Data from the New Zealand National Eye Bank over the past two decades have consistently reported keratoconus as the leading indication for corneal transplantation, accounting for 40-45% of corneal transplants annually3-5. Corneal crosslinking (CXL) is a relatively new technique used to strengthen corneal tissue utilising riboflavin as a photosensitizer and ultraviolet-A light (UVA).
The history of crosslinking
Crosslinking, in general terms, is the creation of bonds that connect polymer chains6. Crosslinking of collagen and elastin molecules was proposed in the 1970s, whereby lysyl oxidase catalysed the formation of crosslinking aldehydes. Then, in 1997, Spoerl et al used this principle in the laboratory to increase corneal stiffness7, and the concept of CXL was born.
Spoerl et al treated porcine eyes with several different protocols using a combination of UVA, blue light, sunlight and 0.5% riboflavin (vitamin B2). Their experiments demonstrated that the combination of riboflavin and UVA successfully increased corneal stiffness by a factor of three7. This technique was then implemented in vivo by Wollensak et al on progressing keratoconus patients in 2003. In their landmark study8, following the removal of the central 8mm of corneal epithelium, riboflavin drops were applied to the cornea for 30 minutes and the eyes irradiated with UVA (370nm, 3mW/cm2) at a 1cm distance for 30 minutes, for a total surface energy exposure of 5.4J/cm2. The treatment stopped the progression of the disease in all eyes, while in 70% of eyes a regression in keratometric and refractive values was observed8. This Wollensak et al method was refined into the standard CXL procedure known as the ‘Dresden protocol’.
Crosslinking today
Recent CXL techniques have departed from this protocol and use different formulations and delivery methods of riboflavin to avoid epithelial debridement (transepithelial CXL), as well as high-intensity UVA exposure (accelerated CXL) to shorten duration times, reduce patient discomfort and minimise postoperative complications, such as infection, haze and endothelial toxicity9.
Epithelial debridement is thought to be a major contributor to postoperative complications such as infective keratitis and abnormal wound-healing response. This piqued interest in the application of epithelium-on or transepithelial CXL. The main challenges associated with this technique are the limited diffusion of riboflavin through the lipophilic cornea and epithelial tight junctions9. The diffusion of riboflavin can be achieved, however, by several techniques, including modifying corneal epithelial permeability, changing the physicochemical properties of the riboflavin molecule and directly delivering riboflavin into the corneal stroma9. Whilst our team at the University of Auckland has reported that the transepithelial CXL technique is effective in stopping the progression of keratoconus, with a follow-up period of two years, it is currently only used in cases where the cornea is too thin to allow for safe epithelium-off CXL (ie. thinnest pachymetry <400μm) as it does not provide the same flattening effect as epithelium-off CXL10.
Accelerated CXL (ACXL) reduces treatment time by utilising the Bunsen-Roscoe law of photochemical reciprocity, which states that the same photochemical effect can be achieved with a reduced irradiation interval, provided total energy is kept constant through a corresponding increase in irradiation intensity11. Our team has actively been involved in researching the outcomes of various crosslinking protocols, with 24 months follow-ups, and has reported better outcomes with the continuous version of the treatment compared to the pulsed technique10. Patients referred to the CXL service at Greenlane are currently offered continuous epithelium-off ACXL or, in the cases of thin corneas, transepithelial CXL.
Ensuring timely CXL treatment
Timely treatment with CXL can prevent visual loss in keratoconus and reduces the need for corneal transplantation3,12. After the introduction of CXL treatment, the frequency for keratoplasties was more than halved in a Swedish unit over a decade13. This is of particular relevance in New Zealand as the lifetime risk of requiring a corneal graft for those with keratoconus is probably higher than the reported 10-20% in the literature14,15. However, most patients are assessed in the community and a recent survey of more than 70 optometrists in Australia suggested that 7% would refer a patient with keratoconus at the time of diagnosis and that a third would only refer on the progression of corneal signs16. To prevent visual loss and allow prompt access to CXL we propose that patients should be referred for CXL if they meet any of the following criteria:
Our group's research has also shown that access to CXL needs to be improved. In a recently published study, we demonstrated that 40% of eyes show evidence of disease progression whilst waiting to undergo CXL, with a mean waiting time of 153 days17. This is significantly higher than the only other similar literature report, a European study in which 25% of eyes demonstrated signs of progression with an average waiting time of 84.8 days18.
Our data also revealed that Māori patients are more likely to show signs of keratoconus progression while waiting for CXL17. This increased risk is in keeping with previous reports of a higher prevalence of keratoconus in Māori patients, an increased likelihood of requiring a corneal transplant as a result of keratoconus and a significantly lower age at the time of surgery compared with Europeans19. The exact cause for significant progression in Māori patients is unknown. Māori patients have previously been reported to have poor attendance at follow-up appointments, independent of social status19.
Our team proposes that a better understanding of referral patterns and the variations in access to treatment by different patient populations can allow for improving access to CXL.
CXL treatment developments
Along with access, we are also working on more effective treatment with better outcomes. Our team’s research, coupled with other publications, demonstrates that CXL can stabilise keratoconus but cannot significantly improve uncorrected distance visual acuity, and can only slightly improve the corrected-distance visual acuity over medium to long-term follow up10. Thus most patients with moderate to advanced disease still need supplemental refractive correction to achieve functional vision.
Therefore, the appeal in combining CXL with adjuvant refractive procedures to provide disease stability, improve functional outcomes and minimize underlying refractive error has been increasing. These ‘CXL plus’ procedures aim to regularise the corneal surface at the time of CXL to provide better visual outcomes in individuals with moderate to advanced keratoconus.
Several CXL plus procedures are reported in the literature and involve the use of excimer laser technology in the form of transepithelial phototherapeutic keratectomy (T-PTK) or photorefractive keratectomy (PRK) to partially regularise the distorted corneal surface immediately before conducting CXL. The excimer laser is widely used in refractive surgery and the use of CXL plus protocols has been reported to be safe and efficacious20-22.
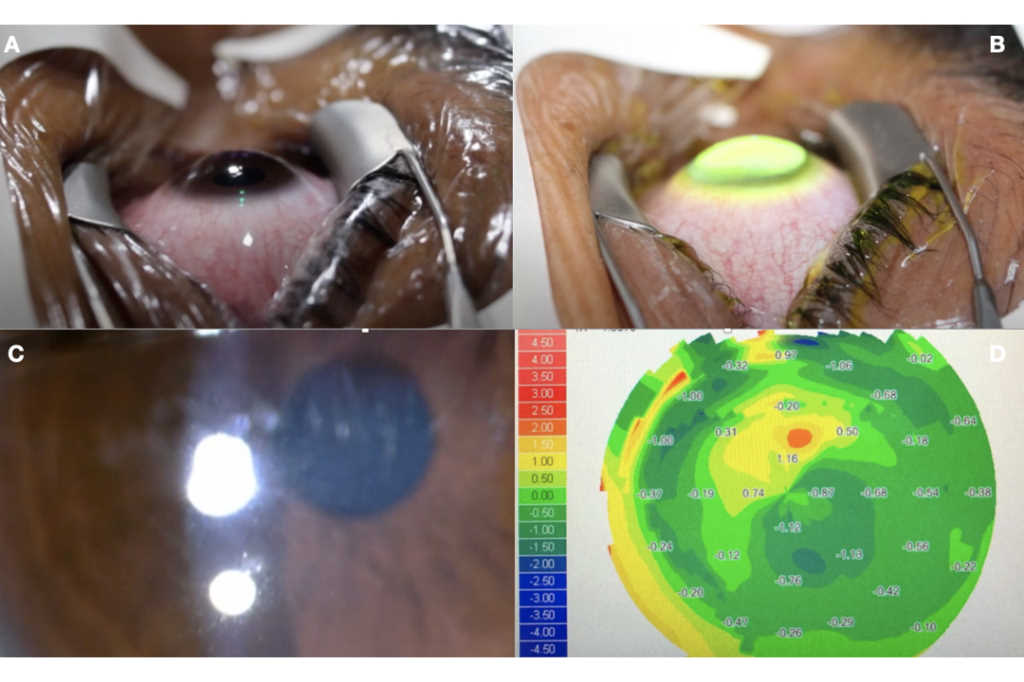
Our team is currently investigating a modified CXL plus protocol which we have termed the ‘Auckland protocol’, which utilises an excimer laser to remove 55μm of tissue centrally and 65μm of tissue peripherally at an 8.0mm optical zone (Fig 1A), followed by CXL using an accelerated protocol (Fig 1B). Initial results indicate that the Auckland protocol can provide several advantages including:
We hope that our ongoing research contributions could ultimately lead to more timely treatment with CXL, which has previously been reported to be a cost-effective intervention25, and potentially reduce the need for more invasive intervention, such as corneal transplantation, and ultimately reduce the public health burden of this disease.
References
Dr Lize Angelo is currently a house officer with the Auckland District Health Board and was the winner of the 2018 Calvin Ring Undergraduate Prize in Ophthalmology
Dr Akilesh Gokul is a therapeutically qualified optometrist, specialising in keratoconus at Mortimer Hirst in Auckland and a research fellow in the Department of Ophthalmology at the University of Auckland
Dr Mo Ziaei is a consultant ophthalmologist specialising in cataract sugery, laser vision correction and transplantation at Greenlane Clinical Centre and Re:Vision in Auckland. He is also a senior lecturer in ophthalmology at the University of Auckland, having completed his doctoral thesis on novel options for the treatment of corneal disease.